Gender Disparities in Sickness Absence Burden Insights from Central and Eastern European Countries
Katarzyna Miszczyńska * 
Piotr Miszczyński *
Summary: This study focused on the gender gap in sickness absenteeism in Central and Eastern European countries from 2010 to 2023. Eurostat data and the shift-share analysis (SSA) method were applied to assess the impact of regional, sectoral and local factors on changes in sickness absenteeism. The findings highlighted variations in the length of sickness absence among European countries, in relation to CEE region’s overall developmental status. Additionally, the study confirmed the significance of the research and the growing issue of the gender gap in sickness absence in CEE countries. The results of the SSA analysis indicate that gender inequalities in sickness absenteeism decreased in most countries during the period studied, but the COVID-19 pandemic increased these differences in some sectors. The study provides important information for policymakers and employers seeking to promote equality in the workplace and improve the health and well-being of employees.
Keywords: gender, gender gap, sickness absence, CEE countries
JEL: I19, J8, J16
Nierówności w obciążeniu absencją chorobową z perspektywy płci w krajach Europy Środkowo-Wschodniej
Streszczenie: Niniejsze badanie skupiało się na analizie różnic płciowych w absencji chorobowej w krajach Europy Środkowo-Wschodniej w latach 2010–2023. W celu oceny wpływu czynników regionalnych, sektorowych i lokalnych na zmiany w absencji chorobowej wykorzystano dane Eurostatu oraz metodę analizy shift-share (SSA). Wyniki badania ujawniły zróżnicowanie długości absencji chorobowej w krajach europejskich w kontekście ogólnego poziomu rozwoju regionu Europy Środkowo-Wschodniej. Ponadto badanie potwierdziło istotność podjętej tematyki oraz narastający problem różnic płciowych w absencji chorobowej w krajach tego regionu. Wyniki analizy SSA wskazują, że nierówności płciowe w absencji chorobowej zmniejszyły się w większości krajów w badanym okresie. Badanie dostarcza istotnych informacji dla decydentów politycznych i pracodawców, którzy dążą do promowania równości w miejscu pracy oraz poprawy zdrowia i dobrostanu pracowników.
Słowa kluczowe: płeć, absencja chorobowa, kraje Europy Środkowo-Wschodniej, luka płciowa
1. Introduction
Employee’s health and sickness absence are critical concerns in contemporary work environments (Hendriksen et al. 2016). The impact of sickness absence is substantial on the overall disease burden throughout Europe, affecting both public health and economic stability (Ármannsdóttir et al. 2013). The burden of disease encompasses a comprehensive array of costs associated with health-related issues. The estimated contribution to GDP losses ranges from 1–4% on average (Miszczyńska et al. 2023), underscoring its significant economic impact on both individuals and the society (Miszczyńska et al. 2023). Employee sickness absence, which leads to diminished labor productivity, can substantially impact productivity costs for employers (Strömberg et al. 2017). Poor health within the workforce is associated with several negative outcomes, including decreased productivity, premature withdrawal from the labor market, heightened healthcare expenditures, reduced tax revenues, increased social welfare costs, greater social exclusion and poverty, and an augmented burden on families and caregivers (de Vroome et al. 2015; Irastorza et al. 2016).
The factors influencing employee sickness absenteeism are multifaceted, encompassing social, demographic, occupational, and cultural elements (Antczak, Miszczyńska 2023). Research on the determinants of employee absenteeism has not only facilitated the development of a comprehensive catalog of these factors (Antczak, Miszczyńska 2021) but has also contributed to the formulation of models that categorize these determinants and elucidate their impact on employee sickness absence (Striker 2016). One of such models is Multi-Facet Gender and Health Model by Bekker (2003).
The model illustrated in Figure 1 was originally developed to categorize the various impacts of biological, psychological, and socio-cultural factors on health-related sex differences. It now specifically focuses on examining sex differences in sickness absence (Bekker et al. 2009). According to the model, the relationship between sickness absence and sex (male or female) is influenced by biological sex differences (such as male or female physiology), gender (the internalized socio-cultural constructs of masculinity and femininity), and several potential mediating factors between gender and the outcome variable (Bekker et al. 2009). These factors include sex differences in daily life and/or social position; gender-specific person-related factors; and gender bias in diagnostics, statistics, common sense, and treatment (Bekker et al. 2009).
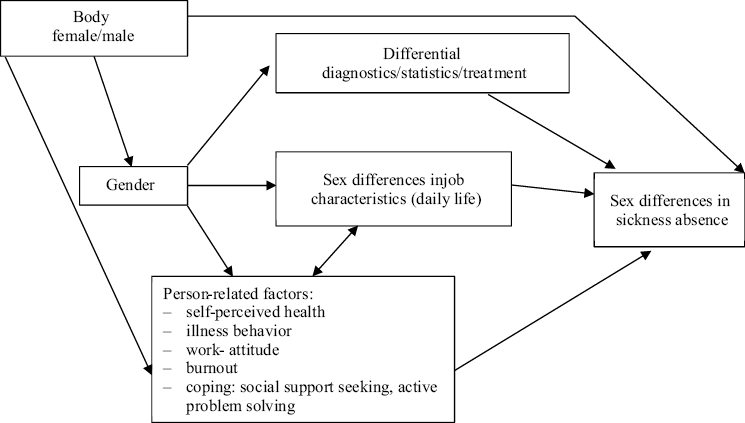
Source: (Bekker et al. 2009)
Gender is a frequently examined factor in the analysis of absentee behaviors. It is commonly utilized as a criterion for data categorization, facilitating subsequent, more detailed analyses. Furthermore, investigations into the gender disparity in sickness absence are conducted, although these are typically confined to individual nations or specific illnesses within a particular country or region (Mastekaasa 2014). Mastekaasa conducted several studies on gender differences in sickness absence from managerial perspective (Mastekaasa et al. 2021), the impact of occupation and workplace on sickness absence (Laaksonen et al. 2010) or sickness absence tolerance (Løset et al. 2018).
The disparity in employee sickness absence across European nations is quite pronounced. This finding is substantiated by a series of studies conducted by Miszczyńska and Antczak (2023). The authors, analyzing the development of sickness absence among employees, observed quite considerable variation in the values of indicators reflecting sickness absence also within the group of CEE countries. The variation in sickness absence patterns among different European countries, including the ostensibly similar Central and Eastern European nations, highlights the diverse healthcare systems, labor market policies, and societal attitudes towards work and health.
Despite the availability of statistical data from government agencies, there is a paucity of studies examining the rate of change in sickness absenteeism, whether in terms of costs incurred or the number of workdays lost, through comparative analyses of a pan-European scope, particularly from the perspective of gender inequalities. Mastekaasa (2014) conducted a study comparing five European countries regarding long-term trends in the gender gap in sickness absence. Similarly, Gimeno et al. surveyed 15 European Union countries using data from the Third European Survey on Working Conditions (Gimeno et al. 2014). In contrast, Antczak and Miszczyńska analyzed the determinants of sickness absence across selected European countries from a gender perspective; however, they did not examine the rates of change (Antczak, Miszczyńska 2021).
Sickness absence represents a financial burden to organizations and the society at large (Nilsen et al. 2017). Although research on the determinants of employee sickness absence is being conducted in many countries, the mechanisms of the gender gap in sickness absence are still not fully understood (Nilsen et al. 2017). Consequently, a research gap has been identified concerning a comprehensive analysis of the rate of change in the number of days of sickness absence across European countries, with a focus on the decomposition of these changes by region and gender. To address this gap, Eurostat data was analyzed and incorporated into a shift-share analysis. The primary objective of this study was to assess the structure of changes in sickness absence in Central-East Europe, particularly in terms of the gender gap. Consequently, the following research questions were identified:
RQ1: How has the duration of employee sickness absence evolved over the analyzed years with respect to gender?
RQ2: In which countries has the gender gap increased, and at the expense of which gender?
RQ3: In which countries did the rate of change in the number of sickness absence days exceed the rate of change across CEE countries?
2. Data and methods
The analysis was conducted utilizing statistical data sourced from the Eurostat database. Consequently, we examined sickness absence among employed individuals, both male and female, aged 20 to 64, across a selected Central – Eastern European countries: Czechia, Estonia, Hungary, Lithuania, Latvia, Poland, Slovakia, Slovenia. The time span of the study is 2010–2023.
Sickness absence, as previously discussed, denotes an employee’s inability to attend work due to personal illness or disability. This phenomenon is of substantial significance not only to employers but also to the economy as a whole, given its effect on GDP (Miszczyńska et al. 2023). Commonly referred to as sickness absenteeism or simply absenteeism, sickness absence is typically quantified as the total number of workdays employees miss due to health-related issues. This definition will be consistently applied in our study. Moreover, the study was conducted from a gender perspective, which is in line with the literature, and was based on Multi-Facet Gender and Health Model by Bekker (2003).
In the study, the SSA’s share shift analysis was incorporated. Originally introduced by E.S. Dunn in 1960, shift share analysis is a weighted decomposition technique designed to disaggregate changes in the structure of both temporal and cross-sectional variables into components of varying nature. As noted by Żółtaszek (2024), SSA effectively determines whether and to what extent these changes are influenced by overarching economic trends (global, national effect), unique regional circumstances (regional, geographic effect), or alterations in the structure of specific sectors (structural, sectoral, cross-sectional effect).
SSA examines the formation of the TX variable quantified in composite form: absolute growth or relative growth (rate of change) of the X variable. Thus, the output data are the txri values of the TX variable, where r is the index corresponding to the r-th region, and subscript i is the index of the i-th group according to the cross-sectional distribution (Suchecki 2010; Trzpiot et al. 2013) . The SSA analysis is conducted in three steps. Firstly, the weights are calculated. In the simplest case, the reference distribution is usually the marginal distribution of the analyzed variable X in the initial period. In the analyses three types of weights can then be used (Suchecki 2010; Trzpiot et al. 2013):
- regional weights
 where
where 
- sectoral weights
 where
where 
- individual weights
 where
where 
Afterwards, to conduct the SSA analysis in addition to determining the individual growth rate of variable X in the i-th sector and in the r-th region  ,
,
where,  is the observation of the analyzed variable X in the r-th region and the i-th group of cross-sectional division in the final period, the following aggregate measures should also be determined (Suchecki 2010; Trzpiot et al. 2013):
is the observation of the analyzed variable X in the r-th region and the i-th group of cross-sectional division in the final period, the following aggregate measures should also be determined (Suchecki 2010; Trzpiot et al. 2013):
- average growth rate of variable X in the r-th region
 ;
; - average growth rate of variable X in the i-th sector
 ;
;  average growth rate of variable X in the country in a given period.
average growth rate of variable X in the country in a given period.
Finally, the pure effect of regional (net regional) growth was calculated

where
 – pure effect (net increase/decrease), surplus/deficit of average rate over the rate of overall;
– pure effect (net increase/decrease), surplus/deficit of average rate over the rate of overall;
 – structural change factor;
– structural change factor;
 – local change factor.
– local change factor.
The analysis was conducted by comparing the phenomenon's level over time through the use of relative increments. Consequently, the changes that occurred during the periods 2010/2015, 2015/2020, and 2010/2020 were examined.
3. Results
The analysis focused on the reference region, specifically the Central and Eastern European countries. Bulgaria was omitted from the study due to insufficient data availability. The calculations incorporated regional weights, expressed as proportions of the variable under examination. The analysis spanned the following time intervals: 2015/2010, 2019/2015, 2023/2019, and the comprehensive period of 2023/2010. In order to capture and verify the existence or not of a gender gap, the analyzed sickness absence was divided into results from a gender perspective. This procedure was in line with the literature and studies conducted by Antczak and Miszczyńska (2021), Kristensen et al. (2010), and Thorsen et al. (2019).
The results were analyzed and presented from two distinct angles. Initially, the focus was on examining the trend in the number of sickness absence days in CEE countries, with a breakdown by gender. Subsequently, the study continued to explore the trend in sickness absence days, considering gender, within the CEE countries under review.
3.1. SSA’s analysis results by region (countries)
Analysis of the number of days of sickness absence by region (CEE countries) made it possible to illustrate the trend in the number of days of sickness absence in individual countries compared to the global trend (CEE countries as a whole), and to show how the values of the structural and regional effects affected this. Detailed results are presented in Table 1.
The Central and Eastern European (CEE) countries under analysis exhibited an upward trend in sick leave days across the following intervals: 2010/2015 – 4.27%, 2015/2019 – 10.23%, and 2019/2023 – 3.68%, culminating in a 19.16% increase over the entire 2010/2023 period. Throughout both the initial sub-period and the overall timeframe (2010/2023), the average rate of change in these countries surpassed the global average for changes in sick leave days. A regional analysis of sick leave days (refer to Table 1) reveals that between 2010 and 2015, four countries experienced a net reduction in sick leave days exceeding 11%, with Romania witnessing a decline of over 23%. In contrast, the subsequent sub-period saw a net increase in sick leave days in most countries. However, during the 2019/2023 period, all countries, except for Estonia, Slovenia, and Slovakia, recorded a net decrease in sick leave days, with Romania experiencing a reduction of more than 30%. The local effect was the primary factor influencing these trends.
| Time span | 2010/2015 | 2015/2019 | 2019/2023 | 2010/2023 | ||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Country [%] | Pure net effect [%] | Structural effect [%] | Local effect [%] | Average rate of change [%] | Pure net effect [%] | Structural effect [%] | Local effect [%] | Average rate of change [%] | Pure net effect [%] | Structural effect [%] | Local effect [%] | Average rate of change [%] | Pure net effect [%] | Structural effect [%] | Local effect [%] | Average rate of change [%] |
| Czechia | 7,2 | 0,2 | 7,0 | 11,5 | 12,0 | 0,1 | 11,9 | 22,2 | –4,5 | 0,2 | –4,6 | 5,8 | 25,0 | 4,3 | 20,7 | 44,1 |
| Estonia | 8,6 | 1,4 | 7,1 | 12,8 | 6,0 | 3,0 | 3,0 | 16,2 | 17,5 | 1,5 | 16,0 | 27,8 | 48,4 | 28,2 | 20,2 | 67,6 |
| Hungary | –15,1 | 0,0 | –15,2 | –10,9 | 8,5 | -0,1 | 8,5 | 18,7 | –1,5 | 0,7 | –2,1 | 8,8 | –4,1 | 0,1 | –4,2 | 15,1 |
| Latvia | 19,9 | 0,5 | 19,4 | 24,2 | –2,8 | 1,3 | –4,1 | 7,4 | –3,0 | 0,6 | –3,6 | 7,2 | 23,9 | 10,7 | 13,1 | 43,0 |
| Lithuania | 36,9 | 1,2 | 35,7 | 41,1 | 1,5 | 1,7 | –0,3 | 11,7 | –1,6 | 0,8 | –2,5 | 8,6 | 52,0 | 23,3 | 28,7 | 71,2 |
| Poland | 8,3 | 0,1 | 8,2 | 12,6 | –7,6 | –0,1 | –7,5 | 2,6 | –6,1 | 0,1 | –6,2 | 4,1 | 1,1 | 2,2 | –1,1 | 20,3 |
| Romania | –23,1 | –1,2 | –21,9 | –18,8 | 0,1 | –1,3 | 1,4 | 10,3 | –30,3 | –1,3 | –29,0 | –20,1 | –47,6 | –24,4 | –23,2 | –28,5 |
| Slovak Republic | –18,7 | 0,4 | –19,1 | –14,5 | 14,5 | 0,6 | 13,9 | 24,8 | 3,9 | 1,0 | 2,8 | 14,1 | 2,6 | 7,0 | –4,4 | 21,8 |
| Slovenia | –11,6 | 0,2 | –11,9 | –7,3 | 10,8 | 0,4 | 10,4 | 21,0 | 5,0 | 0,7 | 4,3 | 15,3 | 10,1 | 4,9 | 5,2 | 29,3 |
| The overall rate of change (global effect) | 4,27 | 10,23 | 3,68 | 19,16 | ||||||||||||
Source: Own elaboration.
Based on the calculation of the pure sector effect on the basis of the analysis of the dynamics of changes in the number of days of sickness absence in the countries of Central and Eastern Europe, it was possible to distinguish the countries where the greatest increase or decrease in the number of days of sickness absence was observed (see Table 1). In the 2010/2015, 2015/20219 and 2019/2023 sub-periods, the dominant factor both in terms of decreases or increases in the number of sickness absence days was the local effect. However, no such trend can be observed in the 2010/2023 sub-period, where the structural effect indicated that absenteeism as measured by the number of days increased the most in Estonia and decreased in Romania. A significant increase in the number of days of sickness absence was also noted in 2010/2015 and in 2010/2023.
3.2. SSA analysis results from a gender perspective
The results of the SSA analysis conducted from a gender perspective are shown in Table 2.
| Time span | brak danych | Female [%] | Male [%] | The overall rate of change (global effect) [%] |
|---|---|---|---|---|
|
2010/2015 |
Pure net effect | –1,5 | 2,2 | 4,3 |
| Structural effect | –2,4 | 3,7 | ||
| Local effect | 1,0 | –1,5 | ||
| Average rate of change | 2,8 | 6,5 | ||
| 2015/2019 | Pure net effect | –19,5 | 28,7 | –2,2 |
| Structural effect | –2,4 | 3,7 | ||
| Local effect | 1,0 | –1,5 | ||
| Average rate of change | 2,8 | 6,5 | ||
| 2019/2023 | Pure net effect | 14,8 | 23,1 | 16,9 |
| Structural effect | 4,7 | 4,7 | ||
| Local effect | 10,2 | 18,4 | ||
| Average rate of change | 12,6 | 20,8 | ||
|
2010/2023 |
Pure net effect | –28,6 | 43,5 | 19,2 |
| Structural effect | –5,2 | 7,9 | ||
| Local effect | –23,4 | 35,6 | ||
| Average rate of change | –9,5 | 62,7 |
Source: Own elaboration.
Throughout three of the four sub-periods examined, the number of days women took off due to illness rose, with the most notable increase occurring in the 2010/2023 sub-period, where there was an average rise of 19.2%. During this same sub-period, the number of sickness absence days for women decreased by up to 9.5%, while the overall trend in Europe showed an average increase of 19.2%. Conversely, in the other sub-periods ending in 2020, there was an average increase ranging from 2.8% to 12.6%. For both genders, it is evident that in each sub-period, the local effect played the most crucial role in determining the net effect, while the structural effect was relatively insignificant.
4. Discussion
Gender significantly influences daily behaviors related to health, such as dietary choices, stress management, and exercise routines. These behaviors, in turn, affect susceptibility to various diseases (Hildt-Ciupińska 2024) and consequently impact rates of sickness absence. Perceptions of health status have been observed to differ between men and women. As highlighted by Gil-Lacruz et al. (2022), self-assessed health and gender vary across different countries and generations. This is a crucial element in shaping health behaviors, which form the foundation for sustaining health and can positively influence disease occurrence, further affected by genetic factors and gender (Mauvais-Jarvis et al. 2020).
Perceiving the relationship between gender and employee sickness absence in this way thus became a particular impetus for conducting the analysis presented in this article. The presented study therefore aimed to analyze the changes in the number of days of sickness absence in individual European countries and to relate these changes to the whole of Europe in the context of the existing gender gap (Antczak, Miszczyńska 2021; Løset et al. 2018; Mastekaasa 2014; Østby et al. 2018; Thorsen et al. 2019). The application of analysis in relation to gender was consistent with other studies on sickness absence as well as with the development of the gender gap itself in the context of employee sickness absence (Mastekaasa 2014; Mastekaasa et al. 2021; Østby et al. 2018).
According to the study’s findings, between 2010 and 2015, four out of nine examined countries experienced a net reduction in sickness absence of more than 11%. Notably, Slovakia and Romania saw declines of over 18% and 23%, respectively. In the following periods (2015/2019 and 2010/2023), most countries observed a net rise in the number of sickness absence days, often surpassing the global impact of changes. This trend was primarily driven by the so-called local effect, indicating that domestic regulations or policies, rather than Europe-wide trends, were responsible for the increase (Heymann et al. 2020).
The length of employee sickness absence increased by more than 19% across the entire analyzed group of CEE countries. Looking at this increase from the gender perspective, sickness absence among women slightly decreased (a drop of about 9%) between 2010 and 2023, while for men it rose by more than 62%. However, in the end, the gender gap in CEE countries flattened out. It only widened in the Czech Republic. Additionally, in most countries, there was a shift in the focal point regarding sickness absence. In 2010, men in CEE countries took sick leave much more frequently, while in 2023 the situation was the opposite.
Analyzing the gender gap between 2010 and 2023, it has been noted that disparities have decreased in most countries. Referring the analysis to 2023, it can certainly be observed that the COVID-19 pandemic, which was not only a crisis in the health sense, but also in the economic sense, played a major role. Although it was formally gone by 2023, its effects are still being felt today. It has affected the functioning of the entire world and thus women and men, but not with equal intensity. As Profeta’s research (Profeta 2021) shows, female employees have been disproportionately and negatively affected by the COVID-19 crisis vis-à-vis their male counterparts. During the coronavirus crisis the service sector, in which women are more often hired, has been the most affected due to the consequent lockdown and social distancing measures. That is why, in this sector, a “she-cession” has emerged (Alon et al. 2020). Analyzing the gender gap between 2019 and 2023, this study notes that the disparity has widened in almost half of the countries. In some countries, including Poland, when a covid was diagnosed, an employee immediately got sick leave for 7 to 14 days, which translated into a significant increase in the number of days of sickness absence (Kobuszewski 2021). During the COVID-19 pandemic, many countries adjusted their internal regulations on wage replacement during sick leave on an ongoing basis (Heymann et al. 2020).
It is important to highlight that while lockdowns and remote work led to a decrease in sickness-related absenteeism, it is crucial to remember that certain sectors and services remained operational, thereby facing a heightened risk of infection (Hsuan et al. 2017). According to Profeta’s study (Profeta 2021), female employees have been disproportionately and adversely impacted by the COVID-19 crisis compared to their male colleagues. The service sector, where women are more frequently employed, has been the hardest hit due to lockdowns and social distancing measures during the pandemic. Consequently, this has led to what is termed a “she-cession” in this sector (Alon et al. 2020).
As mentioned earlier, the magnitude of employee sickness absenteeism in a national perspective, measured, for example, by the number of days on sick leave, depends, among other things, on the gender structure of the country’s workforce. Women tend to have a longer lifespan than men and face fewer life-threatening illnesses (Mastekaasa, Melsom 2014). However, when it comes to most health indicators, women generally fare worse than men, experiencing higher levels of morbidity and psychological distress (Melsom 2015; Østby et al. 2018), more negative perceptions of their own health (United Nations 1988), and increased utilization of health services (Bambra et al. 2009). This important paradox has been highlighted in research on gender inequalities for several decades (Bambra et al. 2009; United Nations 1988). Thus, sickness absence fits into this pattern, for which women are more likely to take leave than men.
According to Østby et al. (2018), one explanation for this phenomenon is the double-burden hypothesis, which highlights that women often face more responsibilities at home compared to men (Østby et al. 2018). This situation can arise when women take time off to care for sick family members, such as children, which increases their exposure to illness and leads to more sick leave. These circumstances not only elevate stress levels – resulting in higher absenteeism (Casini et al. 2013) and adversely affecting their health – but also create a conflict between work and home responsibilities (Nilsen et al. 2017). The identified reasons for the gender disparity in sickness absence may have long-term detrimental effects on women. Østby et al. (2018) mention consequences such as decreased income and career prospects, stigmatization, and prolonged exclusion from the workforce. Another factor contributing to the gender gap is the work-family conflict; however, as Østby notes, there is limited research on this topic (Nilsen et al. 2017).
Occupational health management’s role in addressing gender disparities in sickness absence is often overlooked. Regrettably, there is a scarcity of research examining both the role and impact of activities conducted by occupational health management organizations. These entities play a crucial role, as by proactively tackling potential health issues and fostering overall well-being, companies can cultivate a more resilient workforce and lessen the effects of absenteeism on productivity. Consequently, from a policy standpoint, it is essential to further enhance these efforts, such as by integrating regular health evaluations and wellness programs that cater to the specific needs of diverse employee groups.
5. Conclusions
The research verified the presence of variation in the trends of sickness absenteeism from 2010 to 2023 in Central and Eastern European (CEE) countries. It was established that women were more prone to report sickness absence compared to men. The findings highlighted variations in the length of sickness absence among European countries, in relation to Europe’s overall developmental status. Additionally, the study confirmed the significance of the research and the growing issue of the gender gap in sickness absence in Europe. Consequently, the study contributed to the broader discourse on gender disparities in sickness absenteeism, building upon previous research. This study expanded on earlier findings by incorporating a sample specific to the region.
As for the limitations of the research it should be underlined that the study focused solely on confirming the gender gap in sickness absence and did not explore its causes or solutions. Moreover, extending the study to a larger time frame and including in the analysis the extent of institutional support, or not, introduced in each country would complete the composite vision of the analyzed problem. Another limitation of the study was the lack of data for some countries due to their unavailability in the database used, as well as problems sometimes occurring with the comparability of the data obtained.
Future research should aim to examine the interactions between various factors to develop a more comprehensive model of sickness absence. It is well-known that workforce health impacts not only the immediate work environment but also socio-economic factors on a larger scale. A healthy workforce is associated with increased innovation, competitiveness in global markets, and economic growth.
As for the recommendations resulting from the study, there should definitely be strategies and programs implemented in the countries analyzed, either at the national level or dedicated to specific sectors, to support workers in situations of sickness absence resulting, for example, from the need to care for a family member. Moreover, it is extremely important to promote better health outcomes for workers, which in turn, will reduce income inequality and help build more resilient communities capable of facing future challenges.
In conclusion, the study provides substantial evidence of the existence and extent of the gender gap in sickness absence in the CEE region. Moreover, further research is necessary to better understand the complex nature of gender gap in sickness absence and develop more effective intervention strategies.
Autorzy
* Katarzyna Miszczyńska
* Piotr Miszczyński
References
Alon T., Doepke M., Olmstead-Rumsey J., Tertilt M. (2020), The Impact of COVID-19 on Gender Equality.
Antczak E., Miszczyńska K.M. (2021), Causes of sickness absenteeism in europe – analysis from an intercountry and gender perspective, “International Journal of Environmental Research and Public Health”, 18(22), https://doi.org/10.3390/ijerph182211823
Antczak E., Miszczyńska K.M. (2023), Measuring and Assessing Sick Absence from Work: a European Cross-sectional Study, “Comparative Economic Research”, 26(4): 187–211, https://doi.org/10.18778/1508-2008.26.37
Ármannsdóttir B., Mårdby A.-C., Haukenes I., Hensing G. (2013), Cumulative incidence of sickness absence and disease burden among the newly sick-listed, a cross-sectional population-based study, http://www.biomedcentral.com/1471-2458/13/329
Bambra C., Pope D., Swami V., Stanistreet D., Roskam A., Kunst A., Scott-Samuel A. (2009), Gender, health inequalities and welfare state regimes: A cross-national study of 13 European countries, “Journal of Epidemiology and Community Health”, 63(1): 38–44, https://doi.org/10.1136/jech.2007.070292
Bekker M.H.J., Rutte C.G., Van Rijswijk K. (2009), Sickness absence: A gender-focused review, “Psychology, Health and Medicine”, 14(4): 405–418, https://doi.org/10.1080/13548500903012830
Casini A., Godin I., Clays E., Kittel F. (2013), Gender difference in sickness absence from work: A multiple mediation analysis of psychosocial factors, “European Journal of Public Health”, 23(4): 635–642, https://doi.org/10.1093/eurpub/cks183
de Vroome E.M.M., Uegaki K., van der Ploeg C.P.B., Treutlein D.B., Steenbeek R., de Weerd M., van den Bossche S.N.J. (2015), Burden of Sickness Absence Due to Chronic Disease in the Dutch Workforce from 2007 to 2011, “Journal of Occupational Rehabilitation”, 25(4): 675–684, https://doi.org/10.1007/s10926-015-9575-4
Gil-Lacruz M., Gil-Lacruz A.I., Navarro-López J., Aguilar-Palacio I. (2022), Gender Gap in Self-Rated Health: A Cohort Perspective in Eastern European Countries, “Healthcare”, 10(2): 365, https://doi.org/10.3390/healthcare10020365
Gimeno B., Benavides F.G., Alexanderson K., Abma F.I., Ubalde-López M., Delclos G.L. (2014), Cross-national comparisons of sickness absence systems and statistics: towards common indicators, “European Journal of Public Health”, 24(4): 663–666.
Hendriksen C., Fostervold I., Nilsen V. (2016). Self-perceived health and the impact of psychosocial work factors, [in:] S. Järvelin-Pasanen (ed.), Ergonomics in theory and practice, The University Eastern Finland, pp. 249–253, https://www.researchgate.net/publication/362945559
Heymann J., Raub A., Waisath W., McCormack M., Weistroffer R., Moreno G., Wong E., Earle A. (2020), Protecting health during COVID-19 and beyond: A global examination of paid sick leave design in 193 countries, “Global Public Health”, 15(7): 925–934, https://doi.org/10.1080/17441692.2020.1764076
Hildt-Ciupińska K. (2024), Self-assessment of health and care for health among employed men in Poland, “International Journal of Occupational Safety and Ergonomics”, 30(3): 774–781, https://doi.org/10.1080/10803548.2024.2369395
Hsuan C., Ryan-Ibarra S., DeBurgh K., Jacobson D.M. (2017), Association of Paid Sick Leave Laws With Foodborne Illness Rates, “American Journal of Preventive Medicine”, 53(5): 609–615, https://doi.org/10.1016/j.amepre.2017.06.029
Irastorza X., Malgorzata M., William C. (2016), Second European Survey of Enterprises on New and Emerging Risks (ESENER-2) Overview Report: Managing Safety and Health at Work.
Kobuszewski B. (2021), Sickness absence during the COVID-19 pandemic, “Journal of Education, Health and Sport”, 11(11): 11–24, https://doi.org/10.12775/jehs.2021.11.11.001
Kristensen T.R., Jensen S.M., Kreiner S., Mikkelsen S. (2010), Socioeconomic status and duration and pattern of sickness absence. A 1-year follow-up study of 2331 hospital employees, “BMC Public Health”, 10, https://doi.org/10.1186/1471-2458-10-643
Laaksonen M., Mastekaasa A., Martikainen P., Rahkonen O., Piha K., Lahelma E. (2010), Gender differences in sickness absence – The contribution of occupation and workplace, “Scandinavian Journal of Work, Environment and Health”, 36(5): 394–403, https://doi.org/10.5271/sjweh.2909
Løset G.K., Dale-Olsen H., Hellevik T., Mastekaasa A., Von Soest T., Østbakken K.M. (2018), Gender equality in sickness absence tolerance: Attitudes and norms of sickness absence are not different for men and women, “PLoS ONE”, 13(8), https://doi.org/10.1371/journal.pone.0200788
Mastekaasa A. (2014), The gender gap in sickness absence: Long-term trends in eight European countries, “European Journal of Public Health”, 24(4): 656–662, https://doi.org/10.1093/eurpub/cku075
Mastekaasa A., Melsom A. (2014), Occupational segregation and gender differences in sickness absence: Evidence from 17 European countries, “European Sociological Review”, 30(5): 582–594, https://doi.org/10.1093/esr/jcu059
Mastekaasa A., Dale-Olsen H., Hellevik T., Løset G.K., Østbakken K.M. (2021), Gender difference in sickness absence: Do managers evaluate men and women differently with regard to the appropriateness of sickness absence? “Scandinavian Journal of Public Health”, 49(2): 125–131, https://doi.org/10.1177/1403494819890783
Melsom A.M. (2015), The gender of managers and sickness absence, “SAGE Open”, 5(1), https://doi.org/10.1177/2158244015574208
Miszczyńska K.M., Antczak E., Prevolnik Rupel V. (2023), Estimating the Share of Sickness Absence Costs in Europe’s GDP – A Country, Gender and Time Perspective, “Finanse i Prawo Finansowe”, 1: 9–29, https://doi.org/10.18778/2391-6478.s1.2023.01
Nilsen W., Skipstein A., Østby K.A., Mykletun A. (2017), Examination of the double burden hypothesis-a systematic review of work-family conflict and sickness absence, “European Journal of Public Health”, 27(3): 465–471, https://doi.org/10.1093/eurpub/ckx054
Østby K.A., Mykletun A., Nilsen W. (2018), Explaining the gender gap in sickness absence, “Occupational Medicine”, 68(5): 320–326, https://doi.org/10.1093/occmed/kqy062
Profeta P. (2021), Gender Equality and the COVID-19 Pandemic: Labour Market, Family Relationships and Public Policy, “Intereconomics”, 56(5): 270–273, https://doi.org/10.1007/s10272-021-0997-2
Striker M. (2016), Absencja chorobowa pracowników. Uwarunkowania – kształtowanie – pomiar.
Strömberg C., Aboagye E., Hagberg J., Bergström G., Lohela-Karlsson M. (2017), Estimating the Effect and Economic Impact of Absenteeism, Presenteeism, and Work Environment – Related Problems on Reductions in Productivity from a Managerial Perspective, “Value in Health”, 20(8): 1058–1064, https://doi.org/10.1016/j.jval.2017.05.008
Suchecki B. (2010), Ekonometria przestrzenna: metody i modele analizy danych przestrzennych, Warszawa: C.H. Beck.
Thorsen S.V., Pedersen J., Flyvholm M.A., Kristiansen J., Rugulies R., Bültmann U. (2019), Perceived stress and sickness absence: a prospective study of 17,795 employees in Denmark, “International Archives of Occupational and Environmental Health”, 92(6): 821–828, https://doi.org/10.1007/s00420-019-01420-9
Trzpiot G., Ojrzyńska A., Szołtysek J., Twaróg S. (2013), Use Shift Share Analysis of Changes in the Description of the Structure of Blood Donors in Poland.
United Nations (1988), Sex differentials in life expectancy and mortality in developed countries: an analysis by age groups and causes of death from recent and historical data.
Żółtaszek A. (2024), The Burden Of Disease In The Polish Workforce, “Rynek Pracy”, 4: 44, https://doi.org/10.5604/01.3001.0054.8542