Available online at: https://doi.org/10.18778/1898-6773.87.4.08
 https://orcid.org/0009-0005-7229-8285
https://orcid.org/0009-0005-7229-8285
Department of Biotechnology and Life Science, University of Insubria, Varese, Italy
https://orcid.org/0000-0001-5443-8364
Department of Biotechnology and Life Science, University of Insubria, Varese, Italy
https://orcid.org/0009-0001-3162-7696
Department of Biotechnology and Life Science, University of Insubria, Varese, Italy
Superintendence of Archaeology, Fine Arts and Landscape for the Provinces of Biella, Novara, Verbano-Cusio-Ossola and Vercelli
https://orcid.org/0000-0001-5867-9253
Department of Cultural Heritage, University of Padua
LabDig 3A Academy Association
https://orcid.org/0000-0003-3343-3999
Department of Biotechnology and Life Science, University of Insubria, Varese, Italy
ABSTRACT: Cranial anatomical variations, such as biparietal thinning, offer critical insights into the health and living conditions of ancient populations. Despite the presence of extensive archaeological records, biparietal thinning remains a relatively rare and understudied condition. This review aims to synthesize existing bioarchaeological literature on biparietal thinning, addressing its historical prevalence, geographical distribution, and potential etiologies.
This study integrates data from previous bioarchaeological research supplemented with a new case from skeletal remains excavated at the hypogeal cemetery of Santa Maria Maggiore in Vercelli, Northern Italy. The analysis included macroscopic examination, radiological imaging, and comparative analysis with clinical and paleopathological cases to identify and assess the characteristic features of biparietal thinning.
Our analysis of the skeletal remains of an old adult female individual revealed clear indicators of biparietal thinning. Notably, the thinning was bilateral, with the absence of diploe in the affected areas while maintaining the inner and outer tables of the cranial vault. These findings align with documented cases in the literature and contribute new data to the limited corpus of biparietal thinning cases.
This study underscores the importance of integrating paleopathological findings with modern medical knowledge to enhance the understanding of ancient diseases. The case from Vercelli provides an opportunity to explore the multifactorial origins of biparietal thinning and highlights the necessity of a multidisciplinary approach, combining archaeological, anthropological, and medical perspectives. By presenting this new case, we aim to stimulate further research into biparietal thinning and similar cranial pathologies, enriching the broader narrative of human health evolution.
KEY WORDS: parietal thinning, biparietal osteodystrophy, hypogeal cemetery, skeletal remains, bioarchaeology
The discovery of bilateral symmetrical thinning of parietal bones within skeletal remains in bioarchaeology is a rare occurrence. Despite the abundance of large skull collections from archaeological sites worldwide, only a handful of documented cases exist to date (Henneberg et al. 2002). Nonetheless, across epochs and continents, archaeological and anthropological investigations have unearthed cases of biparietal thinning among ancient human populations. In fact, this condition has been recognized for an extended period of time. Specifically, the earliest descriptions of parietal thinning were documented in the 18th century (Fusco et al. 2020). The prevalence of this condition, as reported by early studies such as Carriere in 1874, with estimated frequency of 0.4% in 1000 dry skulls, suggesting that this alteration is an uncommon occurrence in archaeological skeletal remains (Lodge 1975; Henneberg et al. 2002).
Geographically, archaeological occurrences have been sporadic, with reported cases spanning regions across Europe, including England, France, Italy, Austria, Romania and Spain, and other continents, such as America, Africa and Australia (Smith 1907; Durward 1929; Brothwell 1967; Lodge 1967; Dutta 1969; Arnaud and Arnaud 1976; Mallegni 1977; Bruyn 1978; Breitinger 1983; Ortner and Putschar 1985; Barnes 1994; Campillo 1996; Phillips 2007; Vargovà 2016; Fusco et al. 2020; Tonina et al. 2022; Vasile 2022). This widespread distribution implies that there is no association with any specific geographic region or ancestry (Mann et al. 2017).
The condition of parietal thinning is characterized by a distinct region of severe bone thinning located midway between the sagittal suture and the parietal prominence and typically presents symmetrically and bilaterally, rather than on one side only (Cvetković et al. 2022). The condition was first described in 1783 and has been known by various names over time, including malum senile biparietale, senile biparietal atrophy, biparietal thinning, and biparietal osteodystrophy, with the latter two being more commonly used in contemporary literature (Sandifort 1783; Bruyn 1978; Cvetković et al. 2022). Despite being an uncommon to rare condition in clinic, biparietal thinning is increasingly recognized as significant in forensic contexts. The presence of biparietal thinning can render an individual more susceptible to trauma, particularly if the site of impact involves the regions where the bone is thinnest within the depressions (Mann et al. 2017). Clinically, this condition is often discovered incidentally on imaging, patients may report bilateral scalp depressions, localized pain or sustain skull fractures resulting from falls or trauma (Tsutsumi et al. 2008; Yiu Luk et al. 2010; Sanati-Mehrizy et al. 2020; Yokota et al. 2024).
Modern clinical case records indicate that the majority of parietal thinning cases occur in individuals with a minimum average age of 50 for men and over 60 for women (Yılmaz et al. 2013; Mann et al. 2017; Fusco et al. 2020). Nevertheless, due to the scarcity of archaeological cases, it remains challenging to ascertain whether this condition was more prevalent in ancient populations compared to contemporary times (Henneberg et al. 2002).
Debate persists among researchers regarding the etiology of this phenomenon. Some attribute it to a developmental defect, while others associate it with progressive osteoporosis in the elderly (Ortner and Putschar 1985; Aufderheide and Rodríguez-Martín 1998). Other factor considered through the years, range from constant external pressure on the skull (often mentioned in archaeological studies of ancient Egyptians who wore heavy wigs) to syphilis, gonadal insufficiency and postmenopausal osteoporosis as it is more frequently observed in women (Smith 1907; Epstein 1953; Sanati-Mehrizy et al. 2020; Cvetković et al. 2022). Additionally, parietal thinning has been noted in multiple members of some families, but the hereditary aspect remains inconclusive (Camp and Nash 1994). However, the relationship between parietal thinning and age is notable, with both archaeological and clinical studies indicating a higher incidence in older individuals (Epstein 1953; Tsutsumi et al. 2008; Yiu Luk et al. 2010; Yılmaz et al. 2013; Mann et al. 2017; Fusco et al. 2020; Sanati-Mehrizy et al. 2020; Yokota et al. 2024).
As we investigate the complexities of this condition, numerous questions arise concerning its origins, prevalence and implications for ancient populations. Through the ongoing research and examination of archaeological remains, we aim to enhance the understanding of its significance in the broader context of human health and historical development.
In expanding the array of archaeological discoveries, we also present a new case of bilateral thinning of the parietal bones in a female individual unearthed from the subterranean burial site beneath the Church of Santa Maria Maggiore in Vercelli, Northern Italy, as part of a comprehensive review on this anatomical condition.
The co-cathedral of Santa Maria Maggiore was constructed in the 18th century under the direction of the Jesuits. It replaced the “Santissima Trinità” church and in 1780, it adopted the name of the former Santa Maria Maggiore Basilica that once stood nearby to the south. Underneath the church extends a hypogeal space, inaugurated in 1777 for funerary purposes, which reflects the architectural footprint of the overlying structure. This cemetery remained in use until the early 19th century, reflecting the continuity of funerary practices within this site (Tibaldeschi 1996; Destefanis et al. 2022; Fusco et al. 2023; Licata et al. 2023; Vanni et al. 2024).
The aim of this review is to comprehensively summarize articles that discuss archaeological cases of parietal thinning available on major research platforms.
An initial search was conducted on PubMed using the following keywords: “Biparietal thinning”, “Parietal thinning”, “Bilateral parietal thinning”, “Biparietal osteodystrophy”, “Senile arthropathy”, “Parietal osteodystrophy”, “Biparietal senile disease” and “Malum senile biparietale”. Each entry was initially reviewed through its title and abstract, with further examination of the full text if the term’s usage was unclear. Articles focusing on skeletal biology from an archaeological, anthropological and paleopathological perspective were included. On the other hand, articles that were not authored in English, and that addressed modern clinical and forensic cases, were excluded. The online search was conducted with no limitations on publication date and geographical area.
Subsequently, a secondary search was conducted on Scopus, Google Scholar and Research Gate using the same keywords and inclusion/exclusion criteria.
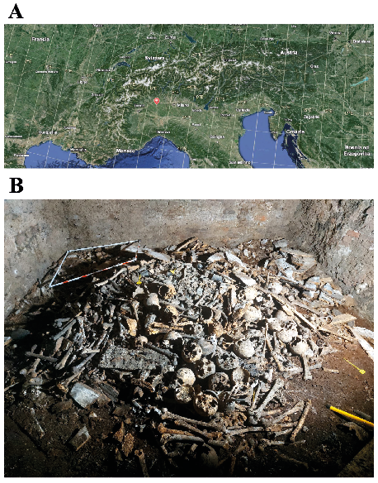
The new case of biparietal thinning, herein presented, originates from the ongoing bioarchaeological investigation at the Church of Santa Maria Maggiore in Vercelli, Piedmont, Northern Italy (Fig. 1.A).
As previously stated, beneath the Church is located a hypogeal cemetery, which was used both for new interments and the relocation of remains from the former complex (Tibaldeschi 1996; Fusco et al. 2023; Vanni et al. 2024).
Figure 1. A) Map of Northern Italy highlighting the location of Vercelli; B) The hypogeal chamber, “Hypogeum 1”.
This vaulted subterranean space contains two underground ossuaries. Bioarchaeological investigations are currently underway in the first ossuary, known as ‘Hypogeum 1’ (Fig. 1.B). It has been divided into square sectors labeled with a combination of numbers (1 to 6) and letters (A to F), and each sector is further subdivided into four corners (North-East, North-West, South-East, South-West) (Fig. 2). This system facilitates the identification of the original location of recovered bones, enabling a more systematic analysis (Orsi et al. 2024).
The cranium featured in this case report was recovered during the early stages of the archaeological investigation. Specifically, it was found in quadrant 1C, Stratigraphic Unit 1, South-East corner (VC SMM24 1C SU1 SE).
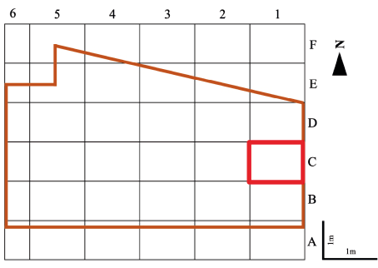
Figure 2. Subdivision of the hypogeum into quadrants with the highlighted square indicating the quadrant (1C) in which the skeletal remain was recovered
To reconstruct the biological profile of the individual, an anthropological analysis was conducted. Sex was determined by observing the diagnostic morphological features of the skull (Buikstra 1994). Age at death was estimated by analyzing the degree of cranial suture closure (Meindl and Lovejoy 1985) and the dental wear (Lovejoy 1985). All available bone measurements were conducted using an electronic digital caliper. Furthermore, a detailed examination of the cranium was performed to identify any pathological conditions. This included macroscopic observations conducted both through unaided visual inspection and with the aid of a magnifying glass. A CT scan was conducted using a Canon Aquilion Start machine with 16/32 slices, following a protocol of 150 mA, 1-second rotation, and 120 kV, with a slice thickness of 0.2 mm. To assess the changes in bone morphology and to measure the bone thickness, the CT scans were analyzed using the Weasis DICOM medical viewer software, version number 4.5.1.0.
The literature review conducted on cases of archaeological biparietal thinning has highlighted several significant findings. The online search across all keywords and search platforms yielded a total of 90.153 hits. The strict selection criteria applied during the review process, focusing exclusively on bioarchaeological and paleopathological contexts, led to the exclusion of most documents, which were predominantly clinical, forensic, or duplicates across platforms. Furthermore, a significant number of articles were excluded due to a lack of relevance to the topic. In addition, several documents were excluded because they were not published in English and not available online, such as Carimati (1954), Piccoli (1965), Kharon and Lifshits (1969) and Takunyacıoğlu (2019). For completeness, in Table 1, we have reported the nine bioarchaeological cases of biparietal thinning that were excluded from the review according to the exclusion criteria (Arnaud and Arnaud 1976; Mallegni 1977; Breitinger 1983; Günay 2005 cited in Çırak 2009; Baggieri 2007; Sağır 2009; Çırak et alt. 2021; Kokotović 2021; Vasile 2022).
Out of all the hits examined through the various search terms and the different search engines, excluding overlapping data (i.e., the same results for different keywords and research platform), only 26 articles (Smith 1907; Durward 1929; Brothwell 1967; Dutta 1969; Bruyn 1978; David 1979; Bartell 1994; Mallegni and Severini 1997; Henneberg et al. 2002; Strouhal et al. 2003; Mulhern 2005; Phillips 2007; Willems et al. 2009; Malnasi 2010; Milsom 2012; Komáry and Fóthi 2013; Seiler and Rühli 2014; Onderka et al. 2015; Vargová et al. 2016; Fusco et al. 2020; Lockwood et al. 2020; Smith et al. 2020; Kozieradzka-Ogunmakin et al. 2021; Tonina et al. 2022; Tornberg 2022; Waziri et al. 2023; Kotze et al. 2024) met the inclusion criteria and therefore they have been included in this review. This corresponds to an exclusion rate of 99.97%, which highlights the rarity of biparietal thinning cases in the archaeological and paleopathological literature available online.
| Site | Chronology | Sex | Age | Diagnosis | Diagnostic method | Literature | Reason for exclusion |
| Ancient Paleocristian Cemetery of the chapel Sancta-Maria de Olivia à Beaulieu | / | M | 50+ | Biparietal thinning | Macroscopic and radiographic analysis | Arnaud and Arnaud 1976 | Not authored in English |
| Eneolithic necropolis of the Gaudo (Paestum), Italy | Eneolithic | F | 50 | Biparietal thinning | Macroscopic and radiographic analysis | Mallegni 1977 | Not authored in English |
| Great pyramid of Cheops | Ancient Egypt | 3 F, 1 M | 30–60 | 4 skulls presenting biparietal thinning | Macroscopic analysis | Breitinger 1983 | Not authored in English |
| Site | Chronology | Sex | Age | Diagnosis | Diagnostic method | Literature | Reason for exclusion |
| Kelenderis, Anatolia | 19th century | M | 60 | Probable case of biparietal thinning | Macroscopic analysis | Günay 2005 cited in Çırak 2009 | Not authored in English |
| Church of San Martino di Ovaro, Udine, Italy | Late Middle Ages | F | 33–49 | Biparietal thinning | Macroscopic and radiographic analysis | Baggieri 2007 | Not authored in English |
| Karaca Ahmet cemetery, Istanbul | Ottoman period | F | 55–60 | Biparietal thinning | Macroscopic analysis | Sağır 2009 | Not authored in English |
| Balatlar Church population in Sinop, Anatolia | 18th century | M | Older | Biparietal thinning | Macroscopic and radiographic analysis | Çırak et al. 2021 | Not authored in English |
| Mukoše site near Goriš moder Dalmatia | 16th century | M | / | Biparietal thinning | Macroscopic analysis | Kokotović 2021 | Not authored in English |
| Middle Byzantine necropolis from Noviodunum-Isaccea Așezare Civilă Est (Tulcea County, Dobruja, Romania) | Medieval Age (11th–13th centuries) | M | 42 | Biparietal thinning | Macroscopic analysis | Vasile 2022 | Not authored in English |
The analysis of the examined cranium, VC SMM24 1C SU1 SE, revealed several notable characteristics (Fig. 3). The neurocranium is largely intact but missing substantial portions of the left parietal and occipital bones, likely due to taphonomic processes.
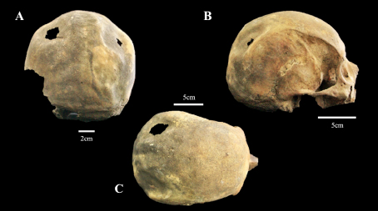
Figure 3. Views of the individual A) posterior view; B) lateral view; C) superior view
The subject was identified as an old adult female (Buikstra 1994), as suggested by the complete ante mortem loss of teeth with significant alveolar resorption and the complete obliteration of all ectocranial sutures.
More detailed observations identified two circular areas of reduced thickness in the cranial table in the upper parietal region, located symmetrically on both sides of the sagittal suture. These areas of biparietal atrophy have the following dimensions: the left area measures 4.65 cm in transverse diameter and 3.62 cm in sagittal diameter while the right area measures 4.47 cm in transverse diameter and 3.1 cm in sagittal diameter. The depth of the thin area on the right side of the skull is 0.56 cm, whereas the depth on the left side cannot be measured due to a central taphonomic hole provoked by the extreme thinness, and therefore delicacy, of the area.
CT images showed bilateral and nearly symmetrical thinning involving the posterior sections of the parietal bones. Furthermore, in the areas unaffected by parietal thinning, the inner and outer tables, along with the diploic space between them, were clearly distinguishable and showed no anomalies. In the transitional zone, a reduction in bone thickness was observed, with the diploe appearing thinner compared to normal bone. Finally, in areas where the trabecular bone was completely resorbed, the inner and outer tables merged to form a thin layer of cortical bone (Fig. 4). The normal cranial bone thickness in unaffected parietal sections measured 5.4 mm, 4.3 mm, and 3.5 mm. In contrast, the thickness in the two resorbed areas was reduced, measuring 2.5 mm, 1.9 mm, and 1.7 mm on the right side, and 3.1 mm, 2.6 mm, and 2.4 mm on the left side.

Figure 4. CT scan of individual in the axial plane, coronal vision. A) Extreme thinning is noted in the right parietal bone, with the absence of diploe and the fusion of the outer and inner tables; B) Progressive thinning of the parietals, with the junction of the outer and inner tables also noted in the left parietal bone; C) Progressive thinning of the parietals, with a taphonomic hole visible in the left parietal bone; D) Stage of thinning in which progressive absence of diploe and fusion of the outer and inner cortices is noted in the right parietal bone
The examination of biparietal thinning in skeletal remains offers significant insights into cranial anatomical variations and provides a broader perspective on historical health. This review, incorporating the newly presented case from the Church of Santa Maria Maggiore in Vercelli, aims to contribute to the understanding of this rare condition.
The literature review highlights the rarity and distribution of biparietal thinning across various historical periods and locations (Smith 1907; Durward 1929; Brothwell 1967; Lodge 1967; Dutta 1969; Arnaud and Arnaud 1976; Mallegni 1977; Bruyn 1978; Breitinger 1983; Ortner and Putschar 1985; Barnes 1994; Campillo 1996; Phillips 2007; Vargovà 2016; Fusco et al. 2020; Tonina et al. 2022). Analysis of reviewed paleopathological cases suggests that although biparietal thinning is infrequent in archaeological settings, it is manifested across a range of populations (Henneberg et al. 2002) (Tab. 2), indicating no clear association with any specific geographic region or ancestry (Mann et al. 2017).
The recently discovered case presented here provides new insights into biparietal thinning. The individual exhibits classic morphological features of parietal thinning such as symmetrical depressions of the parietal bones characterized by a significant thinness of the area (Cvetković et al. 2022), enriching the existing bioarchaeological cases. Notably, this case offers valuable data to increase the understanding of biparietal thinning, particularly in expanding the geographical documentation of this condition within Europe.
| Site | Chronology | Sex | Age (years) | Diagnosis | Diagnostic method | Literature |
| Collection of ancient Egyptian crania | Ancient Egypt, period between the 4th and 19th dynasties | / | / | Cranial thinning | / | Smith GE 1907 |
| Skull collection of the Department of Anatomy, University of Otago, New Zealand (Maori an Moriori, Chinese) | / | 3 M, 2 ND | 25–74 | 5 skulls presenting biparietal thinning | Macroscopic analysis | Durward A 1929 |
| / | Early Britain | / | / | Biparietal thinning | / | Brothwell 1967 |
| Harappa, West Punjab India | 2300 B.C, Bronze Age | F | 45 | Biparietal thinning | Macroscopic analysis | Dutta 1969 |
| Neurological collection, Department of Neuropathology, University Hospital, Leiden, The Netherlands | / | 7 F, 1 M | 51–86 | 8 cases of biparietal thinning | Macroscopic, X-ray and histological analysis | Bruyn1978 |
| Manchester Museum | Ancient Egypt | M | Elderly | Biparietal thinning | Radiographic analysis | David 1979 |
| Naqada, Egypt | Predynastic | / | Middle to older adults | 6 skulls presenting biparietal thinning | Macroscopic analysis | Bartell 1994 |
| Necropolises of Cantone (Collelongo) and Arciprete (Trasacco), Italy | Late Roman Age (1st century B.C., 1st century A.D.) | M | Old adult | Biparietal thinning | Macroscopic and X-ray analysis | Mallegni and Severini 1997 |
| Santa Venera Necropolis of Ancient Poseidonia, Italy | 4th–5th century B.C. | F | >70 | Biparietal thinning | Macroscopic analysis | Henneberg et al. 2002 |
| Abusir, Egypt. Shaft tomb of “Iufaa” | Late 26th dynasty (before 525 B.C.) | M | 25–30 | Biparietal thinning | Macroscopic, radiographic and histological analysis | Strouhal et al. 2003 |
| Western Cemetery at Giza,Egypt | 5th dynasty | M | 27–52 | Biparietal thinning | Macroscopic analysis | Mulhern 2005 |
| Egypt (crania from various museum collections) | Ancient Egypt | / | / | 54 cases of parietal thinning | Macroscopic analysis and CT scan | Phillips 2007 |
| Deir al-Barsha, Egypt | Ancient Egypt (Old Kingdom) | 1 F, 1 M, 1 ND | >30–35 | 3 cases of biparietal thinning | Macroscopic analysis | Willems et al. 2009 |
| Dayr Al-barsha And Sheikh Said, Egypt | Ancient Egypt | 3 F, 6 M, 1 ND | >35 | 10 cases of biparietal thinning | Macroscopic analysis | Malnasi 2010 |
| Southern Saskatchewan, Canada (Adamiak cranium) | Middle and Late Middle Precontact Periods | F | 35–45 | Biparietal thinning | Macroscopic analysis | Milsom, 2012 |
| Material of el-Assasif, Thebes (inv. no. 7357 and 7358) from the Anthropological Collection of the Natural History Museum of Paris | Ancient Egypt, 18th Dynasty | 1 M (inv. no. 7357), 1 F (inv. no. 7358) | Senile | Biparietal thinning (inv. no. 7357) and left parietal thinning (inv. no. 7358) | Macroscopic analysis | Komáry and Fóthi 2013 |
| Geneva Museum of Art and History, Switzerland | Third intermediate period, Thebes, Egypt | F | 40–50 | Biparietal thinning | Macroscopic and radiographic analysis | Seiler and Rühli 2014 |
| Náprstek Museum, Prague | Third Intermediate Period, Egypt most likely Western Thebes | F | 40–50 | Biparietal thinning | Macroscopic and radiographic analysis | Onderka et al. 2015 |
| Cemetery Prague-Zličín | Migration Period (5th century) | F | 45–50 | Right parietal thinning | Macroscopic analysis | Vargová et al. 2016 |
| Cairo, Egypt | Ancient Egypt | M | Elderly | Biparietal thinning | X-ray and CT scan | Fusco et al. 2020 |
| Maidstone Museum (Kent, United Kingdom) | 2700-year-old mummy “Ta-Kush” | F | >40 | Biparietal thinning | Microcomputed-Tomography | Lockwood et al. 2020; Smith et al. 2020 |
| Theban rock-cut Tombs at Sheikh ‘Abd al-Qurna. Tomb TT95 | Ancient Egypt | M | >45 | Biparietal thinning | Macroscopic and X-ray analysis | Kozieradzka-Ogunmakin et al. 2021 |
| Medieval cemetery of Caravate (north Italy) | Medieval Age | F | 45–55 | Biparietal thinning | Macroscopic, radiographic and histological analysis | Tonina et al. 2022 |
| Kyhl bjersbacken, Vellinge parish, Scania | Neolithic-Early Bronze Age | F | >60 | Biparietal thinning | Macroscopic analysis | Tornberg 2022 |
| Rock cut tomb of Penmes at Saqqara, Egypt | Old Kingdom | F | >60 | Biparietal thinning | Macroscopic analysis | Waziri et al. 2023 |
| Site | Chronology | Sex | Age (years) | Diagnosis | Diagnostic method | Literature |
| South Africa (San people) | 19th century (1875) | F | 45–60 | Biparietal thinning | Macroscopic analysis and CT scan | Kotze et al. 2024 |
Descriptions of parietal thinning date back to the 18th century, with the condition referred to by various names such as “biparietal senile disease,” “senile arthropathy,” “biparietal thinning” and “parietal osteodystrophy” (Sandifort 1783; Bruyn 1978; Cvetković et al. 2022). Historically, this condition typically involves the posterior parasagittal regions and presents with an oval or quadrilateral flat shape (Fusco et al. 2020). Cederlund’s 1982 study provided a radiological classification of parietal thinning into three stages: (i) superficial thinning visible as a radiolucent area on tomographic images; (ii) considerable thinning with more than half of the bone substance lost while the diploe remains; and (iii) complete loss of the diploe and external surface. This classification helps to understand the progression of the condition, which initially affects only the outer table, leaving the inner table intact (Cederlund 1982). Bruyn and Bots described two primary forms of biparietal thinning: flat and grooved. The flat type is more commonly documented and features a plane-like depression, while the grooved type features a crater-like depression, typically oval in shape (Bruyn 1978). Reaching a differential diagnosis in our case is challenging; we can only note the presence of bilateral parietal thinning that, according to Cederlund’s classification, can be classified as third-degree bilateral parietal thinning (Cederlund 1982). Furthermore, based on Bruyn’s classification, our case can be identified as the flat type (Bruyn 1978).
Computer tomography typically shows thinning or absence of the lamina corticalis externa, loss of the diploe, and preservation of the lamina corticalis interna (Tonina et al. 2022).
The CT findings of bilateral symmetrical thinning in the posterior sections of the parietal bones align with previously reported cases in both clinical and archaeological literature. A similar pattern was observed in the clinical case reported by Yiu Luk et al. (2010), where computed tomography revealed bilateral and symmetrical parietal bone thinning, primarily attributed to the loss of diploe and thinning of the outer table. This case shares notable similarities with our findings, particularly in the bilateral presentation and the thinning of the diploe.
In the bioarchaeological field, Tonina et al. (2022) documented a more severe progression of bone thinning, where radiological images demonstrated thinning of the diploe to the extent that it reached the inner table, with a complete absence of the outer table. While our finding also shows diploic resorption, the presence of both cortical tables in the affected areas of our case differentiates it from the more extreme thinning observed by authors.
Fusco et al. (2020) similarly reported a case of biparietal thinning, where the external cranial table appeared particularly affected, showing significant reduction and resorption, nearly exposing the diploe. Our findings deviate from this observation, as the affected areas featured the complete resorption of the trabecular bone, showing a thin cortical layer formed by the merging of the inner and outer tables.
Kotze et al. (2024) reported severe calvaria thinning characterized by large depressions, attributed to extreme resorption of the diploe, which led to diminution of both the outer and inner tables. Despite the similarity of presentation with our case, Kotze’s findings demonstrated a more extreme loss of bone integrity, underscoring the variability of biparietal thinning presentations.
In a forensic case, Cvetković et al. (2022) described a progressive thinning of the outer table, which eventually merged with the inner table, leaving the inner table relatively unaffected. This pattern bears striking resemblance to the resorptive process observed in our CT scans, where the trabecular bone loss resulted in the merging of the cortical layers, though our findings also indicate that the diploe in the transitional zones remained somewhat visible, albeit thinner than in unaffected areas.
These comparative cases highlight the variable nature of biparietal thinning across different contexts, whether clinical, forensic, or paleopathological, but also underscore a common theme: the thinning process often involves selective loss of diploic bone, with varying degrees of involvement of the outer and inner cortical tables. The extent and progression of the thinning, as well as the involvement of one or both tables, appear to differ based on individual cases, suggesting variability in the progression and underlying causes of biparietal thinning.
In addition, the results of various bioarchaeological studies highlight differences in the dimensions of biparietal atrophy areas, with some cases showing greater degree of thinning in the right parietal region (Mallegni 1977; Seiler 2014; Fusco et al. 2020; Tonina et al. 2022). In our case, however, it is challenging to make a precise assessment due to taphonomic damage present in the left area of thinning. These dimensional variations may reflect different stages of disease progression, underscoring the need for further research to fully understand the clinical and prognostic implications associated with such differences.
The debate surrounding the causes of biparietal thinning remains unresolved, with theories ranging from developmental defects and osteoporotic conditions to external pressures and genetic predispositions (Smith 1907; Epstein 1953; Cvetković et al. 2022). The case from Vercelli, involving an old adult female, aligns with contemporary clinical observations indicating a higher prevalence in older individuals and in the female gender (Epstein 1953; Dutts 1969; Mann et al. 2017). This correlation supports the hypothesis that age-related bone changes could be a significant contributing factor. Indeed, this condition appears to be associated with the reduction or cessation of sex hormone activity (Epstein 1953). Furthermore, hormonal imbalances can lead to osteoporosis, which is also linked to a deficiency of osteoclasts, a condition found in histopathological analyses in some cases of parietal thinning (Schmidt 1937; Yiu Luk et al. 2010; Sanati-Mehrizy et al. 2020). However, the variability in the proposed causes and the widespread geographical-historical distribution of occurrences, underscores the necessity for further research to clarify the precise etiology in historical contexts.
Documenting biparietal thinning in historical populations enhances the broader comprehension of ancient health conditions. By integrating data from various archaeological sites, such as Vercelli, researchers can discern patterns and potential causes of this condition more effectively. Continued study of such cases not only sheds light on specific pathological conditions but also augments the overall knowledge of ancient human health and disease.
The ongoing challenge lies in further elucidating the causes and implications of biparietal thinning. Future research should prioritize the collection of additional cases from diverse geographical and temporal contexts to identify common factors. Employing advanced imaging techniques and adopting multidisciplinary approaches, incorporating archaeology, anthropology, and medical science, will be crucial in unraveling the complexities of this condition. Furthermore, exploring genetic and environmental factors in conjunction with skeletal evidence could yield a more nuanced understanding of biparietal thinning.
The discovery of a new case from the Church of Santa Maria Maggiore in Vercelli enhances our knowledge of this rare condition. The case study showing typical signs of biparietal thinning, reinforces contemporary clinical observations of its increased prevalence among older populations and the female sex. This alignment suggests that age-related bone changes may play a crucial role in the development of this condition.
However, the diverse hypotheses regarding its causes, ranging from genetic and environmental factors to external pressures, reveal the complexity of biparietal thinning indicating that multiple factors are likely involved. The geographical diversity of documented cases suggests that biparietal thinning was not restricted to any specific population or period. This widespread occurrence points to a multifaceted etiology that warrants further interdisciplinary investigation.
Future research should focus on broadening the scope of paleopathological studies and integrating new methodologies to deepen our understanding of biparietal thinning. By examining a wider range of cases and employing advanced imaging and analytical techniques, researchers can uncover the most probable causes and impacts of this condition. Such efforts will not only advance our knowledge of ancient human health but also contribute to a more nuanced understanding of the factors influencing skeletal pathology across different historical and geographical contexts.
In conclusion, the insights gained from the Vercelli case study and the broader review highlight the importance of continued research into biparietal thinning. Expanding bioarchaeological research and integrating new findings are essential for unraveling the complexities of this rare condition and understanding its implications for ancient human health.
Acknowledgements
We extend our heartfelt thanks to the Fondazione Cassa di Risparmio di Torino for their generous financial support of the bioarchaeological project at the Cemetery of Santa Maria Maggiore in Vercelli. This project was conducted under the scientific guidance of the Soprintendenza Archeologia Belle Arti e Paesaggio per le Province di Biella, Novara, Verbano-Cusio-Ossola e Vercelli. We are also deeply grateful for the invaluable collaboration and assistance from the Ufficio Diocesano per i Beni Culturali Ecclesiastici e l’Edilizia di Culto, Arcidiocesi Vercelli.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Conflict of interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Authors’ contribution
NR: Conceptualization, Investigation, Writing - original draft; RF: Conceptualization, Writing – review & editing; AV: Data Curation, Writing - review & editing; FG: Resources, Visualization, Writing - review & editing focused on archaeological data; AM: Resources, Visualization, Writing - review & editing; ML: Project administrator, Supervision, Writing - review & editing
Arnaud G, Arnaud S. 1976. Un Nouveau Cas d’Amincissement Bipariétal Symetrique. Bulletins et Mémoires de la Société d’Anthropologie de Paris 3 (s.13): 3–14. https://doi.org/10.3406/bmsap.1976.1833
Aufderheide AC, Rodríguez-Martín C. 1998. The Cambridge Encyclopedia of Human Paleopathology. Cambridge: Cambridge University Press.
Baggieri G. 2007. Depressione simmetrica ectocranica parietale in un individuo proveniente dal sepolcro di San Martino di Ovaro, Quaderni Friulani di Archeologia XVII. Available from Quad 17_07.pdf
Barnes E. 1994. Developmental Defects of the Axial Skeleton in Paleopathology. Niwot: University Press of Colorado.
Bartell M K. 1994. Paleopathology od cranial remains from predynastic Naqada, Egypt. A thesis submitted to the Faculty of Graduate Studies and Research in partial fulfillment of the requirements for the degree of Master of Arts in the Department of Anthropology University of Alberta. https://doi.org/10.7939/R34B2XF09
Breitinger E., 1983. Depressio Biparietalis Circumscripta I. Zwei Falle aus dem Avaren Zeitlichen Gräberfeld von Zwolfaxing bei Wein. Archaeologic Austriaca 66: 141–153. https://doi.org/10.3406/bmsap.1983.3884
Brothwell DR. 1967. Biparietal thinning in early Britain. In: Brothwell DR and Sandison AT (eds), Diseases in Antiquity. Springfield: CC Thomas, pp. 413–416. doi:10.1017/S0003598X00034189
Bruyn GW. 1978. Biparietal osteodystrophy. Clin Neurol Neurosurg 80(3):125–148. https://doi.org/10.1016/s0303-8467(78)80035-3
Buikstra JE, Ubelaker D. 1994. Standards for Data Collection from Human Skeletal Remains. Research series no. 44. Fayetteville, NC: Arkansas archaeological survey research series, pp. 54–98.
Camp JD, Nash LA. 1994. Developmental thinness of the parietal bones. Radiology 42:42–47. https://doi.org/10.1148/42.1.42
Campillo D. 1996. Paleopatologia. Los primeros vestigios de la enfermedad. Barcelona: Fundacion Uriach 1838, p.158.
Carimati A. 1954. Il cranio di Ugo Foscolo (1778–1827) e cenni storici sul malum senile biparietale [The cranium of Ugo Foscolo (1778–1827) and historical signs of biparietal senile disease]. Minerva Med. May 30;45(43): Varia; 880–885. Italian. PMID: 13193690.
Cederlund CG, Adnren L, Olivecrona H., 1982. Progressive Bilateral Thinning of the Parietal Bones. Skelet Radiol 8:29–33. https://doi.org/10.1007/bf00361365
Çırak A. 2009. Kelenderis iskeletlerinin paleoantropolojik analizi ve Anadolu toplumları arasındaki yeri [Yayımlanmamış doktora tezi]. Ankara Üniversitesi, Sosyal Bilimler Enstitüsü, Ankara. Available from Kelenderis iskeletlerinin paleoantropolojik analizi ve Anadolu toplumları arasındaki yeri
Çırak M T, Tarhan E, ve Köroğlu G. 2021. Balatlar Kilisesi’nde ileri düzey biparietal osteodistrofi örneği. Antropoloji 42:59–66. https://doi.org/10.33613/antropolojidergisi.939236
Cvetković D, Bracanović D, Djonić D, Živković V, Djurić M, Nikolić S. 2022. Biparietal osteodystrophy: Macroscopic appearance, computed tomography imaging and microarchitectural analysis. Leg Med (Tokyo) 55:102025. https://doi.org/10.1016/j.legalmed.2022.102025
David AR. 1979. The Manchester Museum Mummy Project: Multidisciplinary Research on Ancient Egyptian Mummified Remains, Manchester Museum (University of Manchester), 9780719012938, https://books.google.it/books?id=nmO7AAAAIAAJ, Manchester Museum.
Destefanis E, Garanzini F, Licata M. 2022. L’insula episcopalis di Vercelli tra medioevo ed età moderna: riflessioni su topografia, strutture materiali e dati bioarcheologici. In: M. Milan-ese, editor. Atti del IX Congresso Nazionale di Archeologia Medievale. Sesto Fiorentino; pp. 426–430.
Durward A. 1929. A Note on Symmetrical Thinning of the Parietal Bones. J Anat 63(Pt 3):356–362.
Dutta PC. 1969. Bilateral parietal thinning in a Bronze Age skull. British Medical Journal l (5635):55. https://doi.org/10.1136/bmj.1.5635.55
Epstein BS. 1953. The concurrence of parietal thinness with postmenopausal, senile, or idiopathic osteoporosis. Radiology 60(1):29–35. https://doi.org/10.1148/ 60.1.29
Fusco R, Licata M, Larentis O, Cermesoni B, Ravagnan A, Ciliberti R, et al. 2020. “Mummies outside their closets”. Paleoradiological investigation of Egyptian mummified remains. Forensic Imaging 22:200397. https://doi.org/10.1016/j.fri.2020.200397
Fusco R, Messina C, Tesi C, Vanni A. 2023. “Capta est ne malitia mutaret intelletum eius...”: Study on a natural mummy from an underground cemetery (18–19th century). Med Hist 7:e2023044. Available from https://www.mattioli1885journals.com/index.php/MedHistor/article/view/15140
Günay I. 2005. Mersin-Kelenderis (19.yy) toplumunun sağlık sorunları [Yayımlanmamış yüksek lisans tezi]. Ankara Üniversitesi, Sosyal Bilimler Enstitüsü, Ankara.
Henneberg M, Henneberg RJ, Cipriani M. 2002. Bilateral symmetrical thinning of the parietals in a female from Santa Venera necropolis of ancient Poseidonia, Italy (5th Century BC). Paleopathol Newsl 118:11–15. Available from Henneberg: Bilateral symmetrical thinning of the... - Google Scholar
Kharon NS, Lifshits PS. 1969. Rentgenodiagnostika osoboĭ formy involiutivnykh izmeneniĭ kosteĭ svoda cerepa-malum senile biparietale [Roentgenodiagnosis of a special form of involutive changes in the bones of the vault of the skull-malum senile biparietale]. Vestn Rentgenol Radiol 44(3):75–77.
Kokotović T. 2021. Rezultati antropološke analize ljudskih koštanih ostataka s lokaliteta Mukoše kraj Goriša iz 2020. godine. In: Annales Instituti Archaeologici 17:1. Available from Rezultati antropološke analize ljudskih koštanih ostataka s lokaliteta Mukoše kraj Goriša iz 2021. godine | RIARH - Repozitorij Instituta za arheologiju
Komáry Z, Fóthi E. 2013. Ancient Egyptian skulls from Thebes in the Anthropological Collection of the Natural History Museum of Paris. In: Skulls from el-Assasif Ann Hist Nat 105:259–290. Available from KomaryFothi.indd
Kotze D, Gunston GD, Harris T, He L, Gibbon VE. 2024. Clinical and Anthropological Analyses of a Case From 19th Century South Africa with a Confluence of Uncommon Cranial Pathological Conditions. The Journal of Craniofacial Surgery 35(4):e396–e399. https://doi.org/10.1097/SCS.0000000000010265
Kozieradzka-Ogunmakin I, Meyer S, Seiler R, Rühli F. 2021. Bioarchaeological Studies of Human Remains from TT95. http://doi.org/10.2307/j.ctv2ks6x2n.25
Licata M, Tesi C, Larentis O, Destefanis E, Garanzini F, Ciliberti R, Fusco R. 2023. Elongated styloid process of an autopsied skull from the Cemetery of Saint Maria Maggiore in Vercelli, 18–19th century (Piedmont, northern Italy). Anthropol Anz Ber Uber Biol-Anthropol Lit. https://doi.org/10.1127/anthranz/2023/1671 Epub ahead of print.
Lockwood P, Elliott J, Nelson A, Harris S. 2020. Computed tomography head and facial bones review of a 2700-year-old Egyptian mummy. BJR Case Rep 6(2):20190076. https://doi.org/10.1259/bjrcr.20190076
Lodge T. 1967. Thinning of the parietal bones in early Egyptian populations and its aetiology in the light of modern observations. In: Brothwell DR and Sandison AT (editors), Diseases in Antiquity. Springfield: CC Thomas, pp. 405–412.
Lodge T. 1975. Developmental defects in the cranial vault. British Journal of Radiolology 48 (570):421–434. https://doi.org/10.1259/0007-1285-48-570-421
Lovejoy CO. 1985. Dental Wear in Libben Population: Its Functional Pattern and Role in the Determination of Adult Skeletal Age at The Death. Am J Phys Anthropol 68:47–56. https://doi.org/10.1002/ajpa.1330680105
Mallegni F. 1977. Un Caso dí Assottigliamento Biparíetale Simmetrico in Un Calvario della Necropoli Eneolitico del Gaudo. Atti Societá Toscana di Scienze Naturali, Memorie 83: 31–41. Available from Mallegni F, 1977. Un Caso dí Assottigliamento Biparíetale Simmetrico in Un Calvario della Necropoli Eneolitico del Gaudo. Atti Societá Toscana di Scienze Naturali, Memorie 83:31–41.
Mallegni F, Severini F. 1997. Dental and Skeletal Pathologies of Two Human Samples Buried in the Necropolis of Cantone (Collelongo-AQ) and Arciprete (Ortucchio-AQ), 1st Century BC – 1st Century AD. Anthropologie (Brno) 35(3):251–261.
Malnasi C. 2010. “Paleopathology In Ancient Eygpt: Evidence from The Sites of Dayr Al-barsha And Sheikh Said.” Available from “Paleopathology In Ancient Eygpt: Evidence From The Sites Of Dayr Al-ba” by Cindy Malnasi
Mann RW, Kobayashi M, Schiller AL. 2017. Biparietal Thinning: Accidental Death by a Fall from Standing Height. J Forensic Sci 62(5):1406–1409. https://doi.org/10.1111/1556-4029.13425
Meindl RS, Lovejoy CO. 1985. Ectocranial suture closure: a revised method for the determination of skeletal age at death based on the lateral anterior sutures. Am J Phys Anthropol 68:57–66. https://doi.org/10.1002/ajpa.1330680106
Milsom H. 2012. A paleopathological and mortuary analysis of three Precontact burials from southern Saskatchewan. Thesis Submitted to the College of Graduate Studies and Research in Partial Fulfillment of the Requirements for the Degree of Masters of Arts in the Department of Archaeology and Anthropology University of Saskatchewan Saskatoon. Available from http://hdl.handle.net/10388/ETD-2012-08-678
Mulhern D. 2005. A Probable Case of Gigantism in a Fifth Dynasty Skeleton from the Western Cemetery at Giza, Egypt. Int J Osteoarchaeol 15:261–275. https://doi.org/10.1002/oa.781
Onderka P, Jungová G, Bučil J, Oktábcová L, Pečený J. 2015. Egyptian mummies and coffins in the collections of the Náprstek Museum: Adult human mummies. Annals Of The Náprstek Museum 36(2):23–48. Available from https://publikace.nm.cz/en/periodicals/aotnpm/36-2/egyptian-mummies-and-coffins-in-the-collections-of-the-naprstek-museum-adult-human-mummies
Orsi M, Rossetti N, Taglioretti R, Zito S, Mazzucchi A. 2024. Preliminary study of the point cloud obtained with a low cost structured light scanner of third lower human molars. J Bioarchaeol Res 2(2):e2024009. Available from https://www.mattioli1885journals.com/index.php/JBR/article/view/16172
Ortner DJ, Putschar WGJ. 1985. Identification of Pathological Conditions in Human Skeletal Remains. Washington DC: Smithsonian Institution Press. https://doi.org/10.5479/si.00810223.28.1
Phillips SR. 2007. Cranial anomaly, pathology, or normal variant? Thin parietal bones in ancient Egyptian human remains, Dissertation. Dissertations available from ProQuest. AAI3292064.
Piccoli N. 1965. Il cosiddetto “Malum senile biparietale” [The so-called “Malum senile biparietal”]. Arch Sci Med (Torino) 120(2):107–115.
Sağır M, Özer İ, ve Güleç E. 2009. Osmanlı dönemi kafataslarının paleopatolojik analizi. Arkeometri Sonuçları Toplantısı 24:65–78. http://www.kulturvarliklari.gov.tr/sempozyum_pdf/arkeometri/24_arkeometri.pdf
Sanati-Mehrizy P, Graziano Fd, Naidich T, Taub Pj. 2020. Characterization of Bilateral Parietal Thinning. J Craniofac Surg 31(3):e288–e291. https://doi.org/10.1097/SCS.0000000000006241
Sandifort E. 1783. De sinusatii profundo, in utroque osse verticis observato, in Exercitationes Academicae I, Caput quintum, S and J Luchtmans, Leyden, (Cited by Bruyn and Bots, 1978).
Seiler R, Rühli F. 2014. A unique case of perforated bilateral parietal bone thinning in a Third Intermediate Period Egyptian mummy (Geneva Museum D 0242). The Journal of Egyptian Archaeology 100:467–474. http://www.jstor.org/stable/24644983
Schmidt MB. 1937. Atrophie und Hypertrophie des Knochens einschheßhch der Osteosklerose. Handbuch der speziehen pathologischen Anatomie und Histologie; von O. Lubarsch u F. Henke, IX. Bd., III. Teil. Berlin: Julius Springer. https://doi.org/10.1007/978-3-7091-5998-9_1
Smith GE. 1907. The causation of the symmetrical thinning of the parietal bones in an ancient Egyptians. J Anat Physiol 41:232–233. Available from The Causation of the Symmetrical Thinning of the Parietal Bones in Ancient Egyptians – PMC
Smith K, Roughley M, Harris S, Wilkinson C, Palmer E. 2020. From Ta-Kesh to Ta-Kush: The affordances of digital, haptic visualisation for heritage accessibility. Digital Applications in Archaeology and Cultural Heritage 19:e00159. https://doi.org/10.1016/j.daach.2020.e00159
Strouhal E, Němečková A, Kouba M. 2003. Palaeopathology of Iufaa and persons found besides his shaft-tomb at Abusir (Egypt). Int J Osteoarchaeol 13:331–338. https://doi.org/10.1002/oa.689
Takunyacıoğlu B. 2019. Zeytinliada insanları ve yaşam biçimleri [Yayımlanmamış yüksek lisans tezi]. Sivas Cumhuriyet Üniversitesi, Sosyal Bilimler Enstitüsü, Sivas.
Tibaldeschi G. 1996. La Chiesa di S. Maria Maggiore di Vercelli e l’Assunzione di Paolo Borroni. Bollettino Storico Vercellese 2:131–150.
Tonina E, Larentis O, Tesi C, Fusco R, Campagnolo M, Licata M. 2022. A Severe Case of Biparietal Thinning in a Medieval Skull From a Northern Italy Necropolis. J Craniofac Surg 33(1):70–75. https://doi.org/10.1097/SCS.0000000000007929
Tornberg A. 2022. Beyond the age of 60+. Evidence of an elderly female from the Neolithic-Early Bronze Age using Transition Analysis 3 age estimation. Fornvannen. ornvännen, 117(2), 134–139. Available from Beyond the age of 60+: Evidence of an elderly female from the Neolithic-Early Bronze Age using Transition Analysis 3 age estimation – Lund University
Tsutsumi S, Yasumoto Y, Ito M. 2008. Idiopathic calvarial thinning. Neurol Med Chir 48:275–278. https://doi.org/10.2176/nmc.48.275
Vasile G. 2022. Osteodistrofia biparietală – o manifestare neobișnuită. Asupra unui schelet medieval de pe teritoriul României. Available from Vasile G. 2022. Osteodistrofia biparietală – o manifestare neobișnuită. Asupra unui schelet medieval de pe teritoriul României.
Vanni A, Fusco R, Tesi C, Licata M. 2024. Autopsy or anatomical dissection? Comparative analysis of an osteoarchaeological sample from an 18–19th century hypogeal cemetery (northern Italy). J Archaeoll Sci: Reports 54:104418. https://doi.org/10.1007/s12024-020-00285-6
Vargová L, Horáčková L, Horáková M, Eliášová H, Myšková E, Ditrich O. 2016. Paleopathological, trichological and paleoparasitological analysis of human skeletal remains from the Migration period cemetery Prague-Zličín Interdisciplinaria Archaeologica 7(1):13–32. https://doi.org/10.24916/iansa.2016.1.1
Waziri M, El-Seaidy YM, El-Seaidy M. 2023. The rock-cut tomb of Penmes at Saqqara, Univerzita Karlova, Filozofická fakulta, Czechia. Pražské Egyptologické Studie. ISSN 1801-3899.
Willems H, De Meyer M, Peeters H, Vereecken S, Depraetere D, Dupras T, et al. 2009. Report of the 2004–2005 campaigns of the Belgian mission to Deir al-Barsha. Mitteilungen des Deutschen Archaologischen Instituts – Abteilung Kairo 65:377–432.
Yilmaz MB, Egemen E, Ozbakir B, Tekiner A. 2013. Epidural hematoma after minor trauma on patient with biparietal osteodystrophy. J Korean Neurosurg Soc 53(1):57–58. https://doi.org/10.3340/jkns.2013.53.1.57
Yiu Luk S, Fai Shum JS, Wai Chan JK, San Khoo JL. 2010. Bilateral thinning of the parietal bones: a case report and review of radiological features. Pan Afr Med J 4:7.
Yokota H, Fujita T, Fujimoto K. 2024. Traumatic Brain Injury in Patient with Biparietal Thinning. World Neurosurg 187:99–100. https://doi.org/10.1016/j.wneu.2024.04.053

