Available online at: https://doi.org/10.18778/1898-6773.87.3.04
 https://orcid.org/0000-0002-1903-9592
https://orcid.org/0000-0002-1903-9592
Department of Anthropology, Panjab University, Chandigarh, India
https://orcid.org/0000-0001-5321-0958
Department of Anthropology, Panjab University, Chandigarh, India
ABSTRACT: Human identification has always remained as a main task of forensic anthropology and forensic science for various purposes. The purpose of human identification may vary from legal identity to disaster victim identification, from criminal identity to unidentified deceased identification. The condition, such as putrefaction, charring and mutilation of corpse always become an obstacle during the process of identification. Due to surviving nature of teeth, they may serve as evidence for identification in highly decomposed conditions. Therefore, a cross-sectional study was conducted on 207 participants (93 males and 114 females) in the age range of 21 to 45 years with the aim of two-dimensional facial reconstruction. Dental casts, anthropometric facial measurements and facial photographs were obtained from the participants. Dental measurements were taken on the cast in the laboratory. Statistical analysis revealed a weak but statistically significant correlation between the dental and facial parameters. The geometrical faces and the shapes were reconstructed based on the dental dimensions. The reconstructed facial geometry and shapes were very similar to the true facial geometry and facial shapes of the individual. By improving identification of disaster victims and unidentified deceased, the results of the study can have considerable implications in forensic and medico-legal case-works.
KEY WORDS: facial morphology, facial reconstruction, facial dimensions, dental dimensions, forensic identification, disaster victim identification.
Teeth, which are the hardest part of human body, serve as a crucial identifier for commingled, decomposed, mutilated, charred, skeletonized and putrefied corpses in various disasters and medico-legal scenario (Mohammed et al. 2019; Krishan et al. 2015). Besides being a crucial identifier, according to the INTERPOL teeth are reliable and scientifically grounded evidence used as primary identifier in disaster victim identification (Interpol 2018). The significance of individualistic features e.g., dental restorative work, dental jewelry, metal wiring, metal amalgamation, decorative work, morphological traits (such as peg shaping of incisors, shoveling in incisors, Carabellis’s cusp, occlusion type, groove pattern of molars, hyperdontia, hypodontia, taurodontism etc.), shape and size variations, teeth wearing and dental anomalies has been well established in the literature and in forensic case-work (Madi et al. 2013; Jodalli et al. 2016; Anu et al. 2018; Chitara et al. 2023; Hinchliffe 2011). Similarly, teeth and jaw measurements (e.g., maxillary incisor-incisor distance, inter canine distance, combined width of central incisors, inter- molar distance, inter- premolar distance, dental arch height and so on) have been reported to be individual, sex and population specific (Omar et al. 2018; Filipovic et al. 2016; Banerjee et al. 2016). The importance of morphometric dental traits is related to their value in anthropological, medical and forensic studies (Singh and Bhasin 1968; Jain et al. 2021; Chunhabundit et al. 2013; Jayakrishnan et al. 2021). The association of morphometric dental traits with specific ancestries and ethnic groups was reported by Matis and Zwemer (1971) in Western United States population, Tinoco et al. (2016) in Southeast Brazilian population, Filipovic et al. (2016) in Siberian population and Omar et al. (2018) in Saudi population. These studies may help in allocating a specific population group to unidentified deceased and narrow down the investigation process.
In the past, researchers have strengthened the significance of morphometric dental traits by exploring links and associations between various dimensions of teeth and face (Chunhabundit et al. 2023; Kini and Angadi 2012; Mishra et al. 2016; Alshamri et al. 2023). Similarly, anthropological and forensic studies have explored an ethnic association of various facial measurements and face forms (shape and structure), which helps in finding the similarities and differences in various endogamous populations (Lu and Jain 2004; Jahanshahi 2012; Voegeli et al. 2021). Thus, predicting facial dimensions from teeth dimensions can also aid in identifying the ancestry of unknown deceased.
Moreover, facial and dental correlation can be effectively utilized in facial reconstruction. However, there is a lack of literature addressing facial reconstruction using morphometric dental traits. To address this research gap, the present research aimed to determine a relationship between facial dimensions and dental dimensions. The study also aimed to geometrically approximating the facial shapes and geometry from the predicted facial values using various dental dimensions.
The present cross-sectional study was conducted in Karnal region of the Haryana state in North India. The research population comprised of 207 healthy participants (93 males and 114 females) aged between 21 and 45 years from Haryana state of North India. An informed written consent was taken from all study participants after explaining to them the nature and the purpose of the study. The present study is a part of Ph.D. research conducted in the Department of Anthropology, Panjab University, Chandigarh, India. The ethical approval for the study was obtained from the Panjab University Institutional Ethical Committee (vide approval number: PUIEC 230602-I-114, dated 9th June 2023).
Only study participants with no dental attrition, no oral diseases, no accidental missing teeth were included in the study. Any study participants with a history of restorative and orthodontic dental treatment were excluded from the study.
Having obtained general demographic information of study participants, such as name, age, sex and address, dental casts were prepared by obtaining the impression of the teeth in Neoalgin alginate impression material (i.e., mixing the alginate material with distilled water to make a slurry which is then immediately applied to impression tray and dental impressions were obtained) with the help of impression tray. Afterwards, the obtained dental impression was poured with dental stone (Kalabhai Kalstone plaster class III) by mixing the dental stone and distilled water (i.e., making a slurry). The prepared casts were than taken out from the trey after drying at room temperature (37℃).
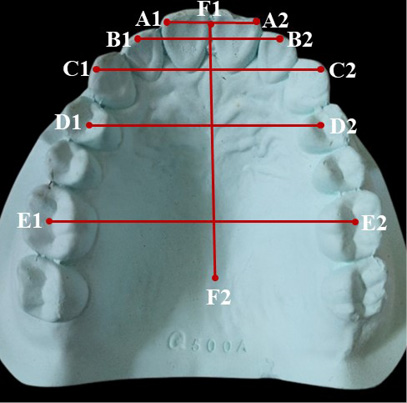
Standardized dental measurements (Zorba et al. 2011; Moreno-Gómez 2013) were recorded from the prepared dental casts with the help of sliding caliper. The dental measurements included in the study are shown in Figure 1 and described in Table 1.
Fig. 1. Dental dimensions included in the study. Distance between A1-A2 = combined width of central incisors, B1-B2 = incisor to incisor distance, C1-C2 = inter canine distance, D1-D2 = inter premolar distance, E1-E2 = inter molar distance, F1-F2 = dental arch height
| FACIAL MEASUREMENTS (Taken directly on the participant’s face following Hall et al. 1989) |
|||
| Sr. No. | Anthropometric Measurement | Description of the measurement | Instrument used |
| 1 | Facial height (FH) | Straight distance from nasion to gnathion in the mid-saggital plane. | Sliding Caliper |
| 2 | Physiognomic facial length (PFL) | Straight distance from trichion to gnathion in the mid-saggital plane. | Sliding Caliper |
| 3 | Maximum head width or Maximum biparietal diameter (MHW) | Distance between right eurion to left eurion. | Spreading Caliper |
| 4 | Minimum frontal breadth (MFB) | Distance between frontotemporalia to frontotemporalia | Spreading Caliper |
| 5 | Upper facial height or Nasal length (UFH) | Distance from nasion to subnasion in the mid-saggital plane. | Sliding Caliper |
| 6 | Lower facial height or Total jaw height (LFH) | Distance from subnasion to gnathion in the mid-saggital plane. | Sliding Caliper |
| 7 | Facial width or Bizygomatic distance (FW) | Distance from right zygion to left zygion. | Spreading Caliper |
| 8 | Inner Canthal distance (ICD) | Distance from right inner canthi to left inner canthi | Sliding Caliper |
| 9 | Outer Canthal distance (OCD) | Distance from right outer canthi to left outer canthi | Sliding Caliper |
| 10 | Nasal width or Interalar distance (NW) | Distance from right alare to left alare. | Sliding Caliper |
| 11 | Mouth width or Intercommissural distance (MW) | Distance between right cheilion and left cheilion | Sliding Caliper |
| 12 | Bigonial distance or Mandible width (BD) | Distance between right gonion to left gonion | Spreading Caliper |
| DENTAL MEASUREMENTS (Taken on the dental cast following Zorba et. al. 2011, Moreno-Gómez, 2013) |
|||
| Sr. No. | Anthropometric Measurement | Description of the measurement | Instrument used |
| 1 | Incisor-Incisor distance (IID) (maxillary) | It is the distance between upper right and upper left lateral incisors. The distance is measured from centre point of lateral incisors. | Sliding Caliper |
| 2 | Inter Canine distance (*ICD) (maxillary) | It is the distance between the cusp tip of upper right and upper left canines. | Sliding Caliper |
| 3 | Combined Width of Central Incisors (CWCI) (maxillary) | It is the combined mesio-distal width of maxillary central incisors. | Sliding Caliper |
| 4 | Inter-Premolar Distance (IPD) (maxillary) | It is the distance from buccal cusp tip of right first premolar to buccal cusp tip of left first premolar. | Sliding Caliper |
| 5 | Inter-Molar Distance (IMD) (maxillary) | It is the distance between buccal groove of right first molar and buccal groove of left first molar. | Sliding Caliper |
| 6 | Dental Arch Height (DAH) | It is the distance/height from occlusal plane of first permanent molar to palatal contour. | Sliding Caliper |
After letting the participants to sit relaxed on a chair and aligning their head in Frankfurt Horizontal plane, various anthropometric landmarks were identified, and dimensions were measured using sliding and spreading caliper in order to obtain various standardized anthropometric measurements. All anthropometric measurements (with their respective landmarks) included in the study are shown in Figure 2 and described in Table 1. Moreover, mid-range facial photographs of all the study participants were taken from a distance of 1 meter using phone’s camera fixed on tripod stand. The photographs of the participants were used for comparison of predicted facial geometry with original facial geometry.
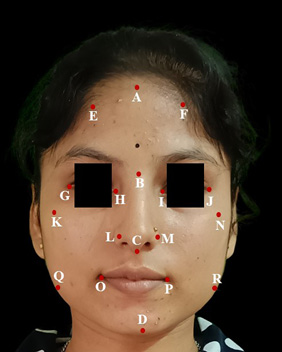
Fig. 2. Anthropometric facial measurements included in the study. Distance between A-D = Physiognomic facial length, B-D = Facial height, B-C = Nasal length, C-D = Total jaw height, E-F = Minimum frontal breadth, G-J = Outer Canthal distance, H-I = Inner Canthal distance, K-N = Bizygomatic distance, L-M = Inter alar distance, O-P = Inter commissural distance, Q-R = Bigonial distance
After entering the data into a computer program MS-Excel, statistical analyses were carried out using the IBM SPSS (Statistical Product and Service Solution) software version 20.0. The following statistical tests were applied to the data in four steps for the fulfillment of objectives of the study:
Step 1: First step involved is the normality assessment of the data, which was carried out by graphical assessment methods (normal Q-Q plots, P-P plots, boxplots), descriptive statistics (mean=mode=median) as well as by confirmatory statistics (Shapiro-Wilk’s test). These tests showed that out of 12 variables 4 variables are normally distributed whereas eight variables are non-normally distributed.
Step 2: In the next step, existence of any correlation between the variables was investigated by applying the parametric test, i.e., Karl Pearson’s correlation coefficient test for normally distributed parameters and non-parametric test, i.e., Spearman’s rank correlation coefficient test for non-normally distributed parameters.
Step 3: In the third step, multiple linear regression models were formulated by step-wise regression method. The stepping criteria for the models were selected as the f-probability between the range of 0.05 to 0.1 (other measurements were excluded). Stepwise regression excludes the insignificantly correlated variables in the model formation and incorporates only those independent variables that significantly explain the dependent variable. This overcomes the issue of overfitting of model and enhances the accuracy and the reliability of the regressions used to fit the models.

Fig. 3. Predicted facial geometry in comparison with true facial geometry of the study participant. A1, B1, C1 and D1 are the true geometry of the study participant (after identifying the anthropological landmarks on the photograph, tracing is drawn in red). A2, B2, C2 and D2 show facial geometry reconstructed from regression models
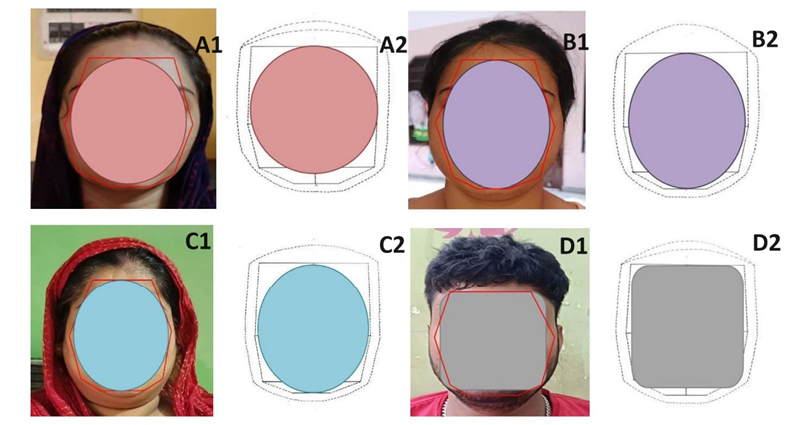
Fig. 4. Predicted facial shape in comparison to the true facial shape of the participant. A1, B1, C1 and D1 show the true facial shapes of the participant (shapes are drawn in color). A2, B2, C2 and D2 show the predicted facial shapes of the participant. Participant A shows an oval face; B and C show a circular face; D shows a squarish facial form
Step 4: Last step in the statistical analysis is the prediction of facial dimensions from the dental dimensions by using regression models. This step provides the outputs of predicted facial dimensions.
Afterwards, facial geometry was drawn manually using a pencil and paper by utilizing the predicted facial dimensions. For bilateral symmetry of the face, the A4 size white bond paper was marked into equal halves (longitudinally and horizontally). The predicted facial measurements of each participant were plotted on the sheet by dividing the measurements into two equal halves and plotted by following the bilateral symmetry. The predicted longitudinal and vertical dimensions of face were plotted on the sheet and joined together to form a facial geometry. For accuracy test the predicted facial geometry and shape was compared manually with original facial geometry and shape (via photographs) (Fig. 3 and 4).
The Shapiro-Wilk’s (95% confidence level) test showed that the physiognomic facial height, outer canthal distance, bigonial distance and inter commissural distance were normally distributed whereas all other parameters, i.e., facial height, maximum head width, minimum frontal breadth, nasal length, bizygomatic distance, total jaw height, inner canthal distance, and interalar distance were non-normally distributed parameters. Table 2 shows the descriptive statistics and Shapiro-Wilk’s test results for normality check.
Further, Table 3 shows the Karl Pearson’s correlation coefficient (for normally distributed variables) and Spearman’s correlation coefficient (for non-normally distributed variables) for assessing the relationship between the facial dimensions and dental measurements. Facial measurements exhibited statistically significant but weak correlation with the dental measurements (Tab. 3). The highest correlation was observed between facial height and IMD (Tab. 3), outer canthal distance and IID (Tab. 3), facial width and IMD (Tab. 3). However, very weak correlation was observed between maximum head width and *ICD, CWCI, IPD, IMD; upper facial height and CWCI; inner canthal distance and CWCI and IPD; lower facial height and *ICD. Beside this, DAH showed insignificant correlation with all the facial measurements except inner canthal distance and nasal width (Tab. 3).
| Anthropometric Measurement | Sample size (N) | Minimum (cms.) | Maximum (cms.) | Mean (cms.) | Standard Deviation (cms.) | Shapiro-Wilk Test | p-value |
| FH | 207 | 9.00 | 12.50 | 10.38 | 0.68 | 0.984 | 0.020 |
| PFL | 207 | 13.90 | 18.80 | 16.44 | 0.93 | 0.995 | 0.684 |
| MHW | 207 | 11.70 | 15.40 | 13.59 | 0.63 | 0.983 | 0.012 |
| MFB | 207 | 9.70 | 13.20 | 11.33 | 0.68 | 0.980 | 0.004 |
| UFH | 207 | 3.90 | 5.70 | 7.74 | 0.37 | 0.979 | 0.004 |
| LFH | 207 | 4.40 | 6.60 | 5.47 | 0.47 | 0.984 | 0.018 |
| FW | 207 | 10.00 | 14.00 | 12.03 | 0.77 | 0.987 | 0.047 |
| ICD | 207 | 2.10 | 3.60 | 2.71 | 0.30 | 0.974 | 0.001 |
| OCD | 207 | 7.30 | 10.30 | 8.87 | 0.54 | 0.989 | 0.111 |
| NW | 207 | 2.70 | 4.20 | 3.38 | 0.31 | 0.977 | 0.002 |
| MW | 207 | 3.60 | 6.10 | 4.83 | 0.50 | 0.988 | 0.093 |
| BD | 207 | 7.90 | 12.90 | 10.35 | 0.97 | 0.991 | 0.193 |
| IID | 207 | 2.60 | 3.50 | 3.01 | 0.19 | 0.965 | <0.001 |
| *ICD | 207 | 2.80 | 3.61 | 3.61 | 0.28 | 0.979 | 0.003 |
| CWCI | 207 | 1.30 | 2.40 | 1.86 | 0.18 | 0.943 | <0.001 |
| IPD | 207 | 3.10 | 4.20 | 3.65 | 0.23 | 0.973 | 0.001 |
| IMD | 207 | 4.00 | 5.50 | 4.82 | 0.29 | 0.976 | 0.002 |
| DAH | 207 | 3.30 | 5.10 | 4.15 | 0.40 | 0.979 | 0.003 |
FH= Facial height, PFL= Physiognomic facial length, MHW= Maximum head width, MFB= Minimum frontal breadth, UFH= Upper facial height, LFH= Lower facial height, FW= Facial width, ICD= Inner Canthal distance, OCD= Outer Canthal distance, NW= Nasal width, MW= Mouth width, BD= Bigonial distance, IID= Incisor-Incisor distance, *ICD= Inter Canine distance, CWCI= Combined Width of Central Incisors, IPD= Inter-Premolar Distance, IMD= Inter-Molar Distance, DAH= Dental Arch Height
| Karl Pearson’s Correlation Coefficient (for normally distributed variables) | ||||||
| Anthropometric measurement | IID | *ICD | CWCI | IPD | IMD | DAH |
| PFL | 0.281** | 0.179** | 0.183** | 0.176** | 0.284** | 0.101 |
| OCD | 0.367** | 0.240** | 0.194** | 0.199** | 0.180** | 0.089 |
| MW | 0.283** | 0.201** | 0.251** | 0.289** | 0.208** | 0.115 |
| BD | 0.207** | 0.183** | 0.156* | 0.195* | 0.277** | -0.015 |
| Spearman’s Rank Correlation Coefficient (for not normally distributed variables) | ||||||
| Anthropometric measurement | IID | *ICD | CWCI | IPD | IMD | DAH |
| FH | 0.208** | 0.134* | 0.223** | 0.281** | 0.369** | 0.058 |
| MHW | 0.191** | 0.077 | 0.075 | 0.130 | 0.105 | -0.012 |
| MFB | 0.274** | 0.116 | 0.257** | 0.184** | 0.245** | 0.081 |
| UFH | 0.167* | 0.174* | 0.065 | 0.166* | 0.205** | 0.026 |
| FW | 0.293** | 0.201** | 0.197** | 0.263** | 0.352** | 0.011 |
| LFH | 0.241** | 0.81 | 0.298** | 0.215** | 0.274** | 0.075 |
| ICD | 0.150* | 0.229** | 0.045 | -0.009 | 0.158* | 0.182* |
| NW | 0.288** | 0.267** | 0.152* | 0.201** | 0.263** | 0.143* |
*p<0.05, **p<0.01; FH= Facial height, PFL= Physiognomic facial length, MHW= Maximum head width, MFB= Minimum frontal breadth, UFH= Upper facial height, LFH= Lower facial height, FW= Facial width, ICD= Inner Canthal distance, OCD= Outer Canthal distance, NW= Nasal width, MW= Mouth width, BD= Bigonial distance, IID= Incisor-Incisor distance, *ICD= Inter Canine distance, CWCI= Combined Width of Central Incisors, IPD= Inter-Premolar Distance, IMD= Inter-Molar Distance, DAH= Dental Arch Height
Regarding correlation coefficients, multiple linear regression models were formulated (95% confidence level) for the prediction of facial dimensions (Tab. 4). The stepping criteria includes the probability of F-to-enter = 0.50, F-to-remove = 0.1. Because of stepwise method of regression formulation, two models (for each parameter) were generated for physiognomic facial height, minimum frontal breadth, total jaw height, bizygomatic distance, inner canthal distance, inter alar distance and inter commissural distance. In contrast, one model for each parameter was formulated for facial height, maximum head width, nasal length, outer canthal distance, and bigonial distance. For assessing the significance of the models’ various other parameters were also calculated, i.e., coefficient of determination (R2), adjusted coefficient of determination or goodness-of-fit (Adj. R2), standard error of estimation (SEE) significance level of model (p-value) (Tab. 4).
| Anthropometric measurement | Regression model | R2 | Adjusted R2 | SEE | p-value |
| Facial height | FH = 6.323+ 0.841 x IMD** | 0.131 | 0.127 | 0.638 | <0.001 |
| Physiognomic facial length | PFL = 12.080+0.905 x IMD** | 0.081 | 0.076 | 0.899 | <0.001 |
| PFL = 10.196+0.666 x IMD**+ 1.007 x IID** | 0.117 | 0.108 | 0.883 | 0.003 | |
| Maximum head width | MHW = 11.568+0.672 x IID** | 0.041 | 0.026 | 0.622 | 0.004 |
| Minimum frontal breadth | MFB = 8.375+0.981 x IID** | 0.073 | 0.069 | 0.664 | <0.001 |
| MFB = 7.146+0.759 x IID**+0.394 x IMD** | 0.098 | 0.089 | 0.657 | 0.004 | |
| Upper facial height | UFH = 3.686+0.219 x IMD** | 0.029 | 0.024 | 0.372 | 0.014 |
| Lower facial height | LFH = 4.141+0.717 x CWCI** | 0.076 | 0.071 | 0.462 | <0.001 |
| LFH = 2.882+0.552 x CWCI**+0.324 x IMD** | 0.111 | 0.103 | 0.454 | 0.003 | |
| Facial width | FW = 7.202+1.001 x IMD** | 0.146 | 0.141 | 0.713 | <0.001 |
| FW = 5.801+0.823 x IM**+0.749 x IID** | 0.175 | 0.167 | 0.703 | <0.001 | |
| Inner canthal distance | ICD = 1.711+0.279 x *ICD** | 0.071 | 0.066 | 0.291 | <0.001 |
| ICD = 2.187+0.362 x *ICD**- 0.213 x IPD** | 0.093 | 0.084 | 0.289 | <0.001 | |
| Outer canthal distance | OCD = 5.692+1.056 x IID** | 0.134 | 0.130 | 0.511 | <0.001 |
| Nasal width | NW = 2.036+0.447 x IID** | 0.071 | 0.067 | 0.307 | <0.001 |
| NW = 1.409+0.334 x IID**+0.201 x IMD** | 0.101 | 0.092 | 0.303 | 0.006 | |
| Mouth width | MW = 2.567+0.753 x IID** | 0.080 | 0.075 | 0.487 | <0.001 |
| MW = 2.269+0.576 x 0.448 x CWCI** | 0.102 | 0.093 | 0.483 | 0.003 | |
| Bigonial distance | BD = 5.924+0.918 x IMD** | 0.077 | 0.072 | 0.93700 | <0.001 |
*p<0.05, **p<0.01, FH= Facial height, PFL= Physiognomic facial length, MHW= Maximum head width, MFB= Minimum frontal breadth, UFH= Upper facial height, LFH= Lower facial height, FW= Facial width, ICD= Inner Canthal distance, OCD= Outer Canthal distance, NW= Nasal width, MW= Mouth width, BD= Bigonial distance, IID= Incisor-Incisor distance, *ICD= Inter Canine distance, CWCI= Combined Width of Central Incisors, IPD= Inter-Premolar Distance, IMD= Inter-Molar Distance, DAH= Dental Arch Height
Further, for evaluating the accuracy and reliability of the models, the mean absolute error (MAE) was assessed for each predicted variable. The formula for calculating the MAE is as follows:
| MAE = | \(\Sigma^{N}_{1}\) Absolute error (AE) |
| Sample size (N) |
Where, absolute error (AE) = Predicted value – True value, sample size (N)= 207
Table 5 depicts the MAE for variables included in the present study. The minimum MAE (-0.0004) was observed for lower facial height whereas the maximum MAE (2.367) was found for upper facial height (Tab. 5). Moreover, for physiognomic facial height both the models have equal MAE (-0.0002). Model 1 was found to be better for minimum frontal breadth, lower facial height, inter alar distance and inter commissural distance model because of lower MAE. However, model 2 was observed to be better for bizygomatic distance and inner canthal distance.
All the predicted facial measurements for each participant were drawn manually with pencil and scale on a standard A4 size white executive bond paper for the reconstruction of facial geometry. The estimation of facial shape was carried out in Microsoft Paint computer program. Figure 3 and 4 show the comparison of facial geometry and facial shape of the participants with the predicted facial geometry and shape. Within the limit of the present study, the predicted facial geometry and shapes were not significantly different from the true facial geometry and shapes. The manual and visual evaluation of predicted and true facial form and geometry was carried out to determine the reliability. It was observed that predicted facial shapes and geometry significantly resembles the true facial shape (Fig. 3 and 4).
| Anthropometric measurement | Absolute error (AE) (Predicted value-true value) |
Mean absolute error (MAE) (AE/Sample size) |
||
| Model 1 | Model 2 | Model 1 | Model 2 | |
| FH | 0.4041 | ---- | 0.0019 | ---- |
| MHW | -0.0272 | ---- | -0.0001 | ---- |
| MFB | -0.0386 | 0.587 | -0.00018 | 0.0028 |
| UFH | 0.0049 | ---- | 2.367 | ---- |
| FW | 0.8 | 0.1419 | 0.0038 | 0.0006 |
| LFH | -0.0963 | -0.5424 | -0.0004 | -0.0026 |
| ICD | 0.1016 | -0.2963 | 0.00049 | -0.0014 |
| NW | -0.2412 | 0.2317 | -0.0011 | 0.0011 |
| PFL | -0.0545 | -0.0566 | -0.0002 | -0.0002 |
| OCD | 0.2104 | ---- | 0.0010 | ---- |
| MW | 0.0422 | 0.3622 | 0.0002 | 0.0017 |
| BD | 0.0704 | ---- | -0.0002 | ---- |
Sample size (N) = 207, FH= Facial height, PFL= Physiognomic facial length, MHW= Maximum head width, MFB= Minimum frontal breadth, UFH= Upper facial height, LFH= Lower facial height, FW= Facial width, ICD= Inner Canthal distance, OCD= Outer Canthal distance, NW= Nasal width, MW= Mouth width, BD= Bigonial distance
The main aim of forensic facial reconstruction is the prediction of the outline, outlook, and appearance of the face of an unknown individual or skull for the purpose of identification. Reconstruction of the face of the individual is an important aspect in case of highly decomposed dead bodies, mutilated and skeletal remains where the face of the dead is beyond recognition. In these cases, anthropologists, odontologists and the forensic scientists opine regarding the identification of the deceased basing on certain preliminary investigations. In the recent past, the scientists have reported facial reconstruction techniques based upon the soft tissue thickness and modeling clay (Bajnoczky and Kiralyfalvi 1995) two- and three-dimensional computerized methods to reconstruction the face (Damas et al. 2020), cranio-facial superimposition technique (Damas et al. 2020; Ubelaker et al. 1992). All these methods either require a complete skull, life-time photograph or sometimes CCTV footage of the deceased. However, this study presents a novel technique for reconstruction of the geometry and shape of the face using dental dimensions. In many mass disaster cases and other forensic caseworks, only jaw and teeth are available as evidence and the present study technique may be utilized so that a clue regarding the facial shapes may help as corroborative evidence along with other techniques of facial reconstruction.
The present study used dental dimensions for the reconstruction of the geometry and facial shape of the individual and compared the outcome with the actual shape and the geometry of the face. Alshamri et al. (2023) also examined the relationship between dimensions of maxillary anterior teeth and face in 150 participants of 18–30 years age range. The study found the significant correlations between inter canthal distance and central incisors, and face width with canine dimensions. Similarly, a highly significant correlation was observed between inner canthal distance and upper canine width in a study conducted by Alaghbari et al. (2023) for the prosthetic dental reconstruction. Kini and Angadi (2013) also carried out a study of correlation between facial dimensions and teeth dimensions on dental cast and smile photograph both for denture aesthetic work. The study revealed that the distance between the tips of the canine (accessed from photograph) is significantly related to inter commissural distance while distance between the tips of the canine (accessed from dental cast) is associates with interpupillary distance.
The outcome of the correlation between studied facial and dental dimensions used in the present study was compared to other analogous studies with similar objective conducted for various purposes (Tab. 6).
| Researcher | Research population and (sample size) | Facial dimensions included | Dental dimensions included | Significant correlation found with dental dimensions | Significant correlation not found with dental dimensions |
| Özdemir and Köseoglu, 2019 | Turkish population (N=210) | ICW, ICD, OCD, IPD, IAD, | Combined mesiodistal width of upper central incisors/2 | ICW, IAD, ICD, OCD | IPD |
| Neda and Garib, 2016 | Kurdish population (N=65) |
IPD, ICD, IAD | CIW, WAT | IPD | IAD, ICD |
| Parciak et al. 2017 | Asian, African, white (N=360) |
BW, IAD, ICD, ICW, IPD | WAT, IW, CW, | ICW | IPD, BW, IAD, ICD |
| Alshamri et al. 2023 | Yemini population (N=150) | ICD, IPD, IAD, ICW, BZW | WAT, CIW, LIW | IPD, ICD, BZW | IAD, ICW |
| Gomes et al. 2006 | Brazilian population (N=81) |
ICD, IPD, IAD, ICW, Eye width | WAT, MCD | ICD, IPD, IAD, ICW, Eye width | ---- |
| Chunhabundit et al. 2023 | Thai population (N=125) |
IPD, ICD, IAD, ICW, BZW, FL, LT | MCD, RIW, LIW, RIH, LIH | IPD. ICD, IAD, ICW, BZW, FL, LT | ---- |
| Present study | North-Indian population (N=207) |
FH, MHW, MFB, UFH, FW, LFH, ICD, NW, PFL, OCD, MW, BD | IID, *ICD, CWCI, IPD, IMD, DAH | MHW, MFB, UFH, LFH, ICD, NW, PFL, OCD, MW, BD | FH, FW, DAH |
IPD= inter pupillary distance, ICD= Inner Canthal distance, OCD= outer Canthal distance, IAD= inter alar distance, ICW= inter commissural width, BZW= Bizygomatic width, FL= face length, LT= lip thickness, CIW= central incisors width (combined), LIW= lateral incisors width, WAT= width of anterior teeth (combined width of centrals, laterals, canines), RIW= right central incisor width, LIW= left central incisor width, RIH= right central incisor height, LIH= left central incisor height, IW= incisor width, CW= canine width, MCD= maxillary canine distance
The results of the present study are also comparable the Mishra et al. (2016) study where weak but significant correlation between combined width of anterior teeth and inter pupillary distance, inter-commissural and inter-alar distance was reported. However, the present study included various other dental and facial variables (Tab. 1) which were not included in the study by Mishra et al. (2016). Nevertheless, some of the other parameters included in the present study were included by Chunhabundit et al. (2023) in a study on Thai population for selection of anterior tooth in orthodontic treatment. The study found that IPD, ICD, ICW and BZW are significantly associated with inter canine distance, right central incisor width, right central incisor height, central incisor height, central incisor width, left central incisor width, left central incisor height in both the sexes. However, this study also revealed sex specific correlation. For instance, lip thickness and Intermedial canthal width were related to dental dimension in women only and face length and lateral canthi to lower border of face distance were related to dental parameters in men only (Chunhabundit et al. 2023).
As far as the prediction of face shape and geometry is concerned, some other researchers explored the association between tooth form and face form for dental prosthetic work and tried to predict the tooth shape from face shape and vice-versa. Koralakunte and Budihal (2012) examined the relation between shape/form of upper right central incisor and face shape/form in 200 (18–29 years) Indian participants. Statistically, they found >50% correlation by visual method and 31.5% correlation by William’s method in the two parameters of their study. Contrasting results were obtained by Mehndiratta et al. (2019) that evaluated the association of face shape and maxillary central incisors in 200 Indian study participants (aged between 18 and 30 years). Non-significant correlation was observed between face shape and tooth shape. Similarly, Wolfart et al. (2004) also reported that there was no association between face and tooth form.
The results of the present study on facial prediction models and the facial geometry and shape approximation can be used in forensic facial reconstruction in medicolegal cases and disaster victim identification. Soft tissue thickness plays an indispensable role in facial reconstruction (Moritsugudi et al. 2022). Anthropological and forensic literature has shown that the soft tissue thickness (STT) exhibits variations with respect to ancestry and sex (Moritsugudi et al. 2022). Therefore, the present study should be extended in the future with appropriate STT (population specific) for more reliable results.
The findings of the present study significantly contribute the forensic and anthropological literature. However, there are some limitations of this study. The present study was based on dental and facial dimensions of Jingar population which is an endogamous group. Therefore, due to anthropological variations in populations the results of the present study are applicable only to the analysed population. Therefore, the authors recommend that similar studies should be conducted on other population groups. The results of the present study are also limited due to the lack of soft tissue thickness (STT) data. The ancestry and sex-based polymorphism in STT concludes that the STT of one population cannot be applied to another population. Moreover, the literature lacks the standardized STT for the study population. The present study did not consider sexual dimorphism while reconstructing the face. Therefore, future studies should include sex variation in facial dimensions and STT, which may lead to more reliable results. Furthermore, the limited sample size of the study also poses a check on the reliability of the results.
The present study was conducted with the aim of estimating the facial geometry and facial shape from the dental measurements. The study observed a weak but significant correlation between the facial and dental dimensions of the variables. Two-dimensional reconstruction of the face (visual and manual examination) in terms of facial geometry and shape was successfully achieved in the present study. The designed facial geometry and shape may be used as a corroborative support in forensic examinations and personal identification along with other methods of forensic facial reconstruction.
Acknowledgements
The principal author (NC) is thankful to the Ministry of Social Justice and Empowerment, Government of India for funding the Ph.D. in the form of a research fellowship. This study is part of the on-going PhD Project of the NC in the Department of Anthropology, Panjab University, Chandigarh, India. KK is supported by the UGC Centre of Advanced Study in Anthropology (CAS II), awarded to the Department of Anthropology, Panjab University, Chandigarh, India.
Ethical approval
The present study is a part of Ph.D. research work in Department of Anthropology, Panjab University, Chandigarh, India. The ethical approval of the study was obtained from the Panjab University Institutional Ethical Committee vide approval number: PUIEC 230602-I-114 dated 09.06.2023. The consent of each participant was also obtained before data collection.
Conflict of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Authors’ contributions
NC – Conceptualization, searching the literature, writing original draft, review and editing, final approval; KK – Writing, review and editing, final approval and supervising the work.
Alaghbari SS, Mohmmed BS, Alalwani NN, Sobhy MM, Qadi KA, Khawaji SA, Mhbob HO, Alsadi FM, Al Moaleem MM. 2023. Analysis of the facial measurements and dental arch dimensions for the construction of dental prostheses among adult Yemenis. J Contemp Dent Pract 24(8):595–604. https://doi.org/10.5005/jp-journals-10024-3511
Alshamri HA, Al-Moaleem MM, Al-Huthaifi BH, Al-Labani MA, Naseeb WR, Daghriri SM, Suhail IM, Hamzi WH, Abu Illah MJ, Thubab AY, Aljabali SA. 2023. Correlation between maxillary anterior teeth and common facial measurements. Clin Cosmet Investig Dent 15:289–300. https://doi.org/10.2147/CCIDE.S438302
Anu V, Arsheya GS, Anjana V, Annison GK, Aruna ML, Alice AP, Aishwarya, BA. 2018. Dental caries experience, dental anomalies, and morphometric analysis of canine among monozygotic and dizygotic twins. Contemp Clin Dent 9(Suppl 2):S314–S317. https://doi.org/10.4103/ccd.ccd_345_18
Bajnoczky I, Kiralyfalvi L. 1995. A new approach to computer-aided comparison of skull and photograph. Int J Legal Med 108(3):157–161. doi: 10.1007/BF01844829.
Banerjee A, Kamath VV, Satelur K, Rajkumar K, Sundaram L. 2016. Sexual dimorphism in tooth morphometrics: An evaluation of the parameters. J Forensic Dent Sci 8(1):22–27. https://doi.org/10.4103/0975-1475.176946
Chitara N, Rani D, Kanchan T, Krishan K. Odontoma and other congenital dental anomalies: Implications for forensic identification. Congenit Anom 63(5):132–140. https://doi.org/10.1111/cga.12533
Chunhabundit P, Prateepamornkul P, Arayapisit T, Teavirat N, Tanachotevorapong P, Varrathyarom P, Srimaneekarn N. 2023. Two-dimensional facial measurements for anterior tooth selection in complete denture treatment. Heliyon 9(10):e20302. https://doi.org/10.1016/j.heliyon.2023.e20302
Damas S, Cordón O, Ibáñez O. 2020. Handbook on craniofacial superimposition: The MEPROCS project. 1st ed. New York: Springer Nature.
Filipovic G, Kanjevac T, Cetenovic B, Ajdukovic Z, Petrovic N. 2016. Sexual dimorphism in the dimensions of teeth in a Serbian population. Coll Antropol 40(1):23–28. PMID: 27301233.
Gomes VL, Gonçalves LC, Do Prado CJ, Junior IL, De Lima Lucas B. 2006. Correlation between facial measurements and the mesiodistal width of the maxillary anterior teeth. J Esthet Restor Dent 18(4):196–205. https://doi.org/10.1111/j.1708-8240.2006.00019_1.x
Hall JG, Froster-Iskenius UG, Allanson JE. 1989. Hand Book of normal physical measurements. Oxford: Oxford University Press.
Hinchliffe J. 2011. Forensic odontology, part 1. Dental identification. Br Dent J 210:219–224.
INTERPOL. 2018. Disaster Victim Identification Guide. [cited 2023 Nov 2023]. Available from https://www.interpol.int/en/How-we-work/Forensics/Disaster-Victim-Identification-DVI
Jahanshahi M. 2012. Ethnicity and Facial Anthropometry. In: Handbook of Anthropometry: Physical Measures of Human Form in Health and Disease. New York: Springer Nature.
Jain A, Saxena A, Jain S, Parihar AP, Rawat A. 2021. Prevalence of developmental dental anomalies of number and size in Indian population according to age and gender. Int J Clin Pediatr Dent 14(4):531–536. https://doi.org/10.5005/jp-journals-10005-1980.
Jayakrishnan JM, Reddy J, Kumar RV. 2021. Role of forensic odontology and anthropology in the identification of human remains. J Oral Maxillofac Pathol 25(3):543–547. https://doi.org/10.4103/jomfp.jomfp_81_21
Jodalli PS, Panchmal GS, Sonde L, Somaraj V. 2016. Heterogeneous occlusal traits among monozygotic twins from the village of twins–A report of 3 cases. Ann Int Med Dent Res 2(6):DE19–23. https://doi.org/10.21276/aimdr.2016.2.6.DE4
Kini AY, Angadi GS. 2013. Biometric ratio in estimating widths of maxillary anterior teeth derived after correlating anthropometric measurements with dental measurements. Gerodontology 30(2):105–111. https://doi.org/10.1111/j.1741-2358.2012.00648.x
Koralakunte PR, Budihal DH. 2012. A clinical study to evaluate the correlation between maxillary central incisor tooth form and face form in an Indian population. J Oral Sci 54(3):273–278. https://doi.org/10.2334/josnusd.54.273
Krishan K, Kanchan T, Garg AK. Dental evidence in forensic identification–An overview, methodology and present status. Open Dent J 9:250–256. https://doi.org/10.2174/1874210601509010250
Lu X, Jain AK. 2004. Ethnicity identification from face images. In: Proceedings of SPIE 5404:114–123. https://doi.org/10.1117/12.542847
Madi HA, Swaid S, Al-Amad S. 2013. Assessment of the uniqueness of human dentition. J Forensic Odontostomatol 31(1):30–39. PMID: 24776439.
Matis JA, Zwemer TJ. 1971. Odontognathic discrimination of United States Indian and Eskimo groups. J Dent Res 50(5):1245–1248. https://doi.org/10.1177/00220345710500052501
Mehndiratta A, Bembalagi M, Patil R. 2019. Evaluating the association of tooth form of maxillary central incisors with face shape using AutoCAD software: A descriptive study. J Prosthodont 28(2):e469–e472. https://doi.org/10.1111/jopr.12707
Mishra MK, Singh RK, Suwal P, Parajuli PK, Shrestha P, Baral D. 2016. A comparative study to find out the relationship between the inner inter-canthal distance, interpupillary distance, inter-commissural width, inter-alar width, and the width of maxillary anterior teeth in Aryans and Mongoloids. Clin Cosmet Investig Dent 8:29–34. https://doi.org/10.2147/CCIDE.S87837
Mohammed F, Fairozekhan AT, Bhat S, Menezes RG. 2019. Forensic Odontology. Treasure Island: StatPearls Publishing.
Moreno-Gómez F. 2013. Sexual dimorphism in human teeth from dental morphology and dimensions: A dental anthropology viewpoint. In: Sexual Dimorphism. London: InTech.
Moritsugudi DS, Fugiwara FV, Vassallo FN, Mazzilli LE, Beaini TL, Melani RF. 2022. Facial soft tissue thickness in forensic facial reconstruction: Impact of regional differences in Brazil. PLos ONE 17(7):e0270980. https://doi.org/10.1371/journal.pone.0270980
Neda AK, Garib BT. 2016. Selecting maxillary anterior tooth width by measuring certain facial dimensions in the Kurdish population. J Prosthet Dent 115(3):329–334. https://doi.org/10.1016/j.prosdent.2015.08.012
Omar H, Alhajrasi M, Felemban N, Hassan A. 2018. Dental arch dimensions, form and tooth size ratio among a Saudi sample. Saudi Med J 39(1):86–91. https://doi.org/10.15537/smj.2018.1.21035
Özdemir H, Köseoğlu M. 2019. Relationship between different points on the face and the width of maxillary central teeth in a Turkish population. J Prosthet Dent 122(1):63–68. https://doi.org/10.1016/j.prosdent.2018.11.006
Parciak EC, Dahiya AT, AlRumaih HS, Kattadiyil MT, Baba NZ, Goodacre CJ. 2017. Comparison of maxillary anterior tooth width and facial dimensions of 3 ethnicities. J Prosthte Dent 118(4):504–510. https://doi.org/10.1016/j.prosdent.2016.10.035
Singh IP, Bhasin MK. 1968. Anthropometry. Delhi: Kamla Raj Enterprises.
Tinoco RL, Lima LN, Delwing F, Francesquini JrL, Daruge JrE. 2016. Dental anthropology of a Brazilian sample: Frequency of nonmetric traits. Forensic Sci Int 258:102–e1–e5. https://doi.org/10.1016/j.forsciint.2015.10.019
Ubelaker DH, Bubniak E, O’Donnell G. 1992. Computer-assisted photographic superimposition. J Forensic Sci 37:750–762.
Voegeli R, Schoop R, Prestat-Marquis E, Rawlings AV, Shackelford TK, Fink B. 2021. Cross-cultural perception of female facial appearance: A multi-ethnic and multi-centre study. PLos ONE 16(1):e0245998. https://doi.org/10.1371/journal.pone.0245998
Wolfart S, Menzel H, Kern M. 2004. Inability to relate tooth forms to face shape and gender. Eur J Oral Sci 112(6):471–476. https://doi.org/10.1111/j.1600-0722.2004.00170.x
Zorba E, Moraitis K, Manolis SK. 2011. Sexual dimorphism in permanent teeth of modern Greeks. Forensic Sci Int 210(1–3):74–81. https://doi.org/10.1016/j.forsciint.2011.02.001

